Y-Hassan Shams
Coronary Artery Disease Area, Heart and Vascular Theme, Karolinska Institutet and Karolinska University Hospital, Stockholm S-141 86, Sweden.
World J Cardiol. 2020 Jun 26;12(6):231-247. doi: 10.4330/wjc.v12.i6.231.
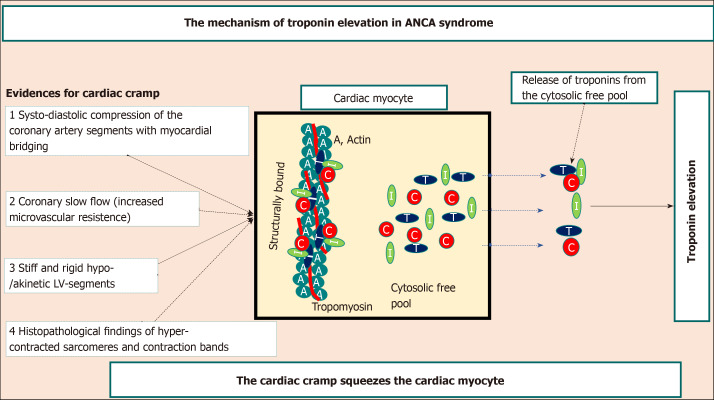
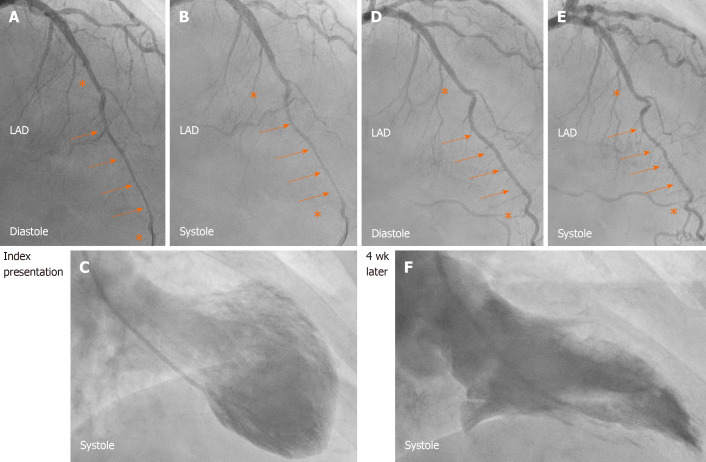
Myocardial infarction (MI) is defined as myocardial cell death due to prolonged myocardial ischemia. Clinically, troponin rise and/or fall have become the "defining feature of MI" according to the universal definition of MI (UD-MI). Takotsubo syndrome (TS) and TS-related disease conditions also cause troponin elevation with typical rise and/or fall pattern but through a mechanism other than coronary ischemia. By strict application of the clinical diagnostic criteria for type-1 MI, type-2 MI, type-3 MI, and MI with non-obstructive coronary arteries according to the UD-MI including the fourth one published recently, TS and most of the 26 other causes of troponin elevation mentioned in the fourth UD-MI may erroneously be classified as MI. The existing evidence argues for the case that TS by itself is not a MI. Hyper-activation of the autonomic-sympathetic nervous system including local cardiac sympathetic hyper-activation and disruption with nor-epinephrine churn and spillover is the most probable cause of TS. This autonomic neuro-cardiogenic (ANCA) mechanism results in myocardial "cramp" (stunning), the severity and duration of which depend on the degree of the sympathetic-hyperactivation and nor-epinephrine spillover. The myocardial cramp may squeeze the cytosolic free troponin pools causing mild to moderate troponin elevation in TS and TS-related disease conditions. This ANCA syndrome, which has hitherto been enveloped by the UD-MI over more than one decade, may occur in acute, recurrent, and chronic forms. In this critical review, the controversies of UD-MI, evidence for ANCA syndrome, and a hypothetical mechanism for the troponin elevation in ANCA syndrome are provided.
心肌梗死(MI)定义为由于长时间心肌缺血导致的心肌细胞死亡。临床上,根据心肌梗死的通用定义(UD-MI),肌钙蛋白升高和/或降低已成为“心肌梗死的决定性特征”。Takotsubo综合征(TS)及与TS相关的疾病状态也会导致肌钙蛋白升高,呈现典型的升高和/或降低模式,但却是通过冠状动脉缺血以外的机制。按照UD-MI严格应用1型心肌梗死、2型心肌梗死、3型心肌梗死及非阻塞性冠状动脉心肌梗死的临床诊断标准(包括最近发布的第四版),TS以及第四版UD-MI中提到的其他26种肌钙蛋白升高原因中的大多数可能会被错误地归类为心肌梗死。现有证据支持TS本身并非心肌梗死这一观点。自主交感神经系统的过度激活,包括局部心脏交感神经的过度激活以及去甲肾上腺素的紊乱和溢出,是TS最可能的原因。这种自主神经源性(ANCA)机制导致心肌“痉挛”(顿抑),其严重程度和持续时间取决于交感神经激活和去甲肾上腺素溢出的程度。心肌痉挛可能挤压细胞溶质游离肌钙蛋白池,导致TS及与TS相关疾病状态下肌钙蛋白轻度至中度升高。这种迄今为止在十多年里一直被UD-MI所掩盖的ANCA综合征,可能以急性、复发性和慢性形式出现。在这篇批判性综述中,提供了UD-MI的争议、ANCA综合征的证据以及ANCA综合征中肌钙蛋白升高的假设机制。