Graham Ryan C, Bush Weston J, Mella Jeffrey S, Fridell Jonathan A, Ekser Burcin, Mihaylov Plamen, Kubal Chandrashekhar A, Mangus Richard S
Department of Anesthesia, University of Utah, Salt Lake City, UT, USA.
Department of Surgery, Mayo Clinic Jacksonville, Jacksonville, FL, USA.
Ann Transplant. 2020 Aug 11;25:e920630. doi: 10.12659/AOT.920630.
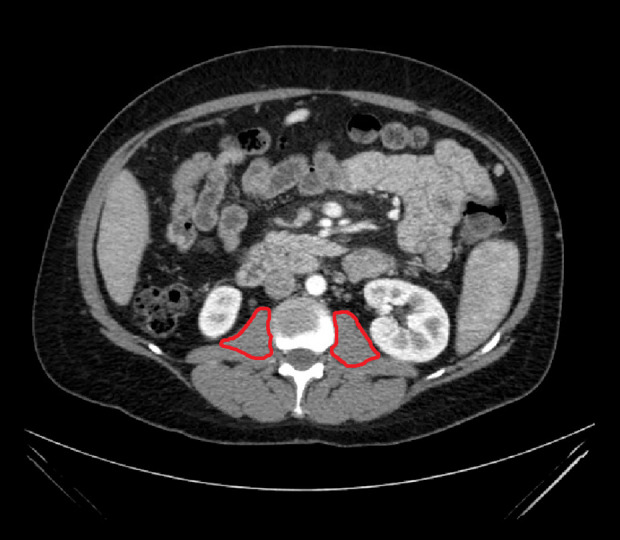
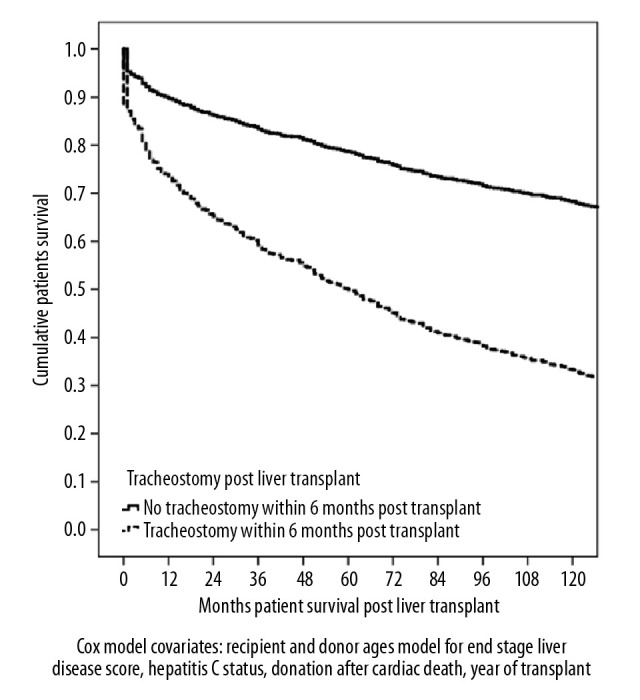
BACKGROUND Liver transplant (LT) patients have an increased risk of postoperative respiratory failure requiring tracheostomy. This study sought to characterize objective clinical predictors of tracheostomy. MATERIAL AND METHODS The records for 2017 LT patients at a single institution were reviewed. Patients requiring tracheostomy were first compared with all other patients. A case-control subgroup analysis was conducted in which 98 tracheostomy patients were matched with 98 non-tracheostomy LT patients. For the case-control study, muscle mass was assessed using preoperative computed tomography scans. RESULTS Among 2017 LT patients, 98 required tracheostomy (5%), with a 19% complication rate. Tracheostomy patients were older and had a higher model for end-stage liver disease score, a lower body mass index (BMI), and a greater smoking history. Tracheostomy patients had a longer hospital stay (45 vs. 10 days, P<0.001) and worse 1-year survival (65% vs. 91%, P<0.001). Ten-year Cox regression patient survival for tracheostomy patients was significantly worse (32% vs. 68%, P<0.001). In the case-control analysis, respiratory failure patients were older (P<0.01) and had a lower BMI (P=0.05). They also had a muscle mass deficit of -39% compared with matched LT controls (P<0.001). No significant differences were seen with pre-LT total protein or albumin or with forced expiratory volume in 1 s divided by forced vital capacity (FEV1/FVC) values. CONCLUSIONS Predictors for respiratory failure requiring post-LT tracheostomy include higher model for end-stage liver disease score, older age, lower BMI, greater smoking history, and worse sarcopenia. Patients requiring tracheostomy have dramatically longer hospital stays and worse survival.
背景 肝移植(LT)患者术后发生呼吸衰竭并需要气管切开术的风险增加。本研究旨在确定气管切开术的客观临床预测因素。材料与方法 回顾了一家机构2017例LT患者的记录。首先将需要气管切开术的患者与所有其他患者进行比较。进行了病例对照亚组分析,其中98例气管切开术患者与98例非气管切开术LT患者进行匹配。对于病例对照研究,使用术前计算机断层扫描评估肌肉质量。结果 在2017例LT患者中,98例需要气管切开术(5%),并发症发生率为19%。气管切开术患者年龄较大,终末期肝病评分较高,体重指数(BMI)较低,吸烟史较长。气管切开术患者住院时间更长(45天对10天,P<0.001),1年生存率更差(65%对91%,P<0.001)。气管切开术患者的10年Cox回归患者生存率明显更差(32%对68%,P<0.001)。在病例对照分析中,呼吸衰竭患者年龄较大(P<0.01),BMI较低(P=0.05)。与匹配的LT对照组相比,他们的肌肉质量也有-39%的 deficit(此处原文可能有误,推测为“减少”)(P<0.001)。LT术前总蛋白或白蛋白以及1秒用力呼气量除以用力肺活量(FEV1/FVC)值未见显著差异。结论 LT术后需要气管切开术的呼吸衰竭预测因素包括终末期肝病评分较高、年龄较大、BMI较低、吸烟史较长以及肌肉减少症更严重。需要气管切开术的患者住院时间显著更长,生存率更差。