Department of Population Family and Reproductive Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
Maternal and Child Health Bureau, Health Resources and Services Administration, Rockville, Maryland, United States of America.
PLoS One. 2020 Aug 11;15(8):e0237314. doi: 10.1371/journal.pone.0237314. eCollection 2020.
Compared to other racial/ethnic groups, infant mortality rates (IMR) are persistently highestamong Black infants in the United States, yet there is considerable regional variation. We examined state and county-level contextual factors that may explain regional differences in Black IMR and identified potential strategies for improvement.
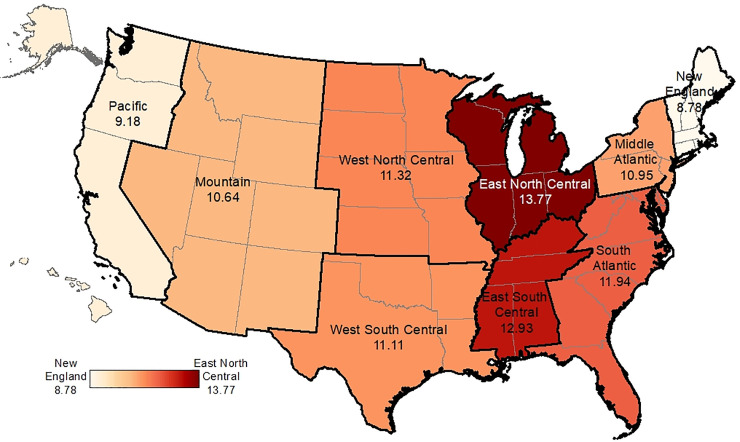
Black infant mortality data are from the Linked Birth/Infant Death files for 2009-2011. State and county contextual factors within social, economic, environmental, and health domains were compiled from various Census databases, the Food Environment Atlas, and the Area Health Resource File. Region was defined by the nine Census Divisions. We examined contextual associations with Black IMR using aggregated county-level Poisson regression with standard errors adjusted for clustering by state. Overall, Black IMR varied 1.5-fold across regions, ranging from 8.78 per 1,000 in New England to 13.77 per 1,000 in the Midwest. In adjusted models, the following factors were protective for Black IMR: higher state-level Black-White marriage rate (rate ratio (RR) per standard deviation (SD) increase = 0.81, 95% confidence interval (CI):0.70-0.95), higher state maternal and child health budget per capita (RR per SD = 0.96, 95% CI:0.92-0.99), and higher county-level Black index of concentration at the extremes (RR per SD = 0.85, 95% CI:0.81-0.90). Modeled variables accounted for 35% of the regional variation in Black IMR.
These findings are broadly supportive of ongoing public policy efforts to enhance social integration across races, support health and social welfare program spending, and improve economic prosperity. Although contextual factors accounted for about a third of regional variation, further research is needed to more fully understand regional variation in Black IMR disparities.
与其他种族/族裔群体相比,美国黑人婴儿的婴儿死亡率(IMR)一直居高不下,但存在相当大的地区差异。我们研究了可能解释黑人 IMR 地区差异的州和县级背景因素,并确定了改善的潜在策略。
黑人婴儿死亡率数据来自 2009-2011 年的链接出生/婴儿死亡档案。社会、经济、环境和健康领域的州和县级背景因素来自各种人口普查数据库、食品环境地图集和区域卫生资源文件。区域由九个人口普查区定义。我们使用按州聚类调整后的标准误差汇总县级泊松回归来检查与黑人 IMR 的背景关联。总体而言,黑人 IMR 在各地区差异 1.5 倍,从新英格兰的每千人 8.78 例到中西部的每千人 13.77 例不等。在调整后的模型中,以下因素对黑人 IMR 有保护作用:较高的州一级黑人和白人结婚率(每标准差增加的比率比(RR)为 0.81,95%置信区间(CI):0.70-0.95)、较高的州母婴健康预算人均(RR 每 SD = 0.96,95% CI:0.92-0.99)和较高的县级黑人群体极端集中指数(RR 每 SD = 0.85,95% CI:0.81-0.90)。模型化变量解释了黑人 IMR 地区差异的 35%。
这些发现广泛支持正在进行的公共政策努力,以加强种族间的社会融合,支持健康和社会福利计划支出,并提高经济繁荣。尽管背景因素仅解释了黑人 IMR 地区差异的三分之一左右,但需要进一步研究以更全面地了解黑人 IMR 差异的地区差异。