Department of Reproductive Health and Health Services Management, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia.
Interdisciplinary School of Health Sciences, Faculty of Health Sciences, University of Ottawa, Ottawa, Canada.
BMC Public Health. 2020 Aug 11;20(1):1222. doi: 10.1186/s12889-020-09297-x.
In Ethiopia, there is a paucity of studies on inequality in caesarean section using methodologically rigorous and well-established approaches. In this study, we showed extent and the overtime dynamics of inequality in caesarean section in Ethiopia following rigorous methodologies.
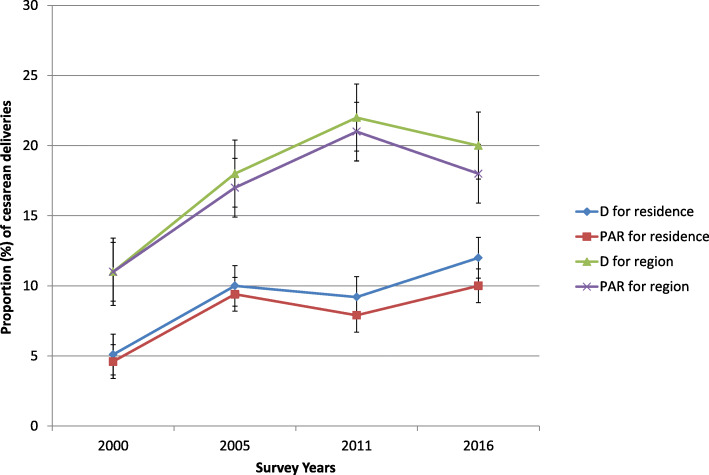
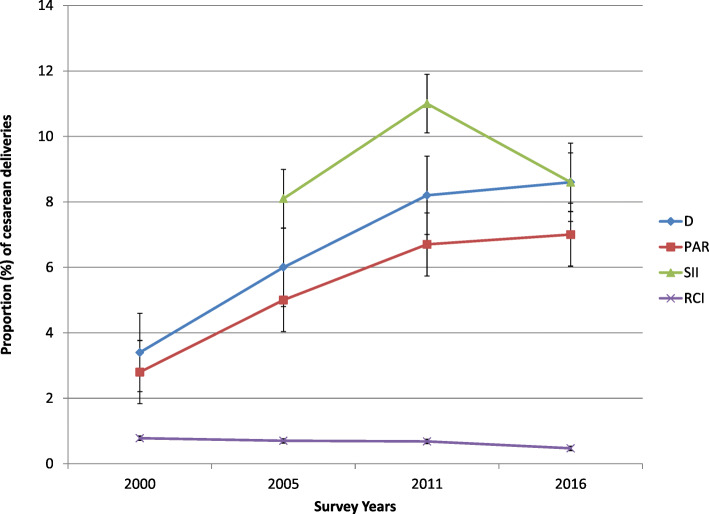
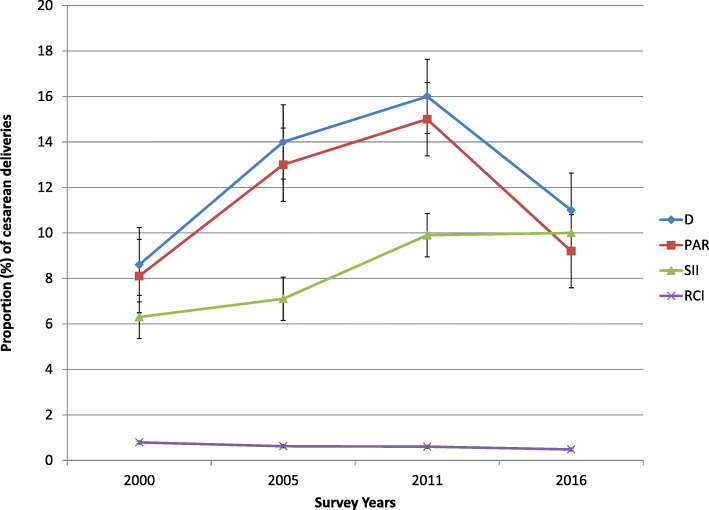
The data for analysis came from Ethiopia Demographic and Health Surveys (EDHS) conducted between 2000 and 2016. We used the World Health Organization's (WHO) Health Equity Assessment Toolkit (HEAT) to analyze the data. Caesarean delivery was disaggregated by four equity stratifiers, namely education, wealth, residence and regions. Relative and absolute summary measures were calculated for each equity stratifier to capture inequality from different perspectives. 95% Uncertainty Interval was calculated around a point estimate to measure statistical significance.
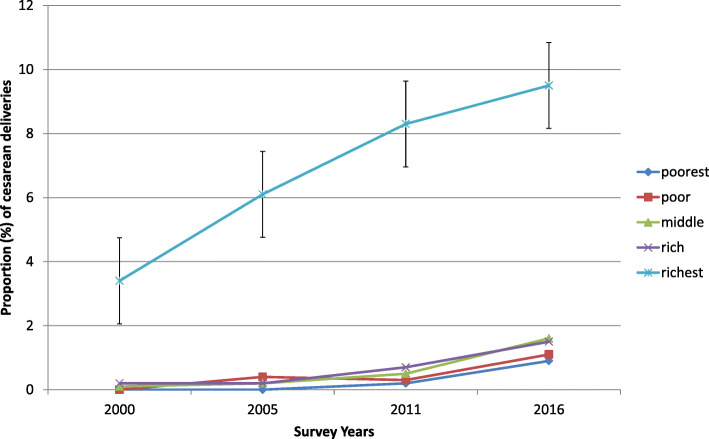
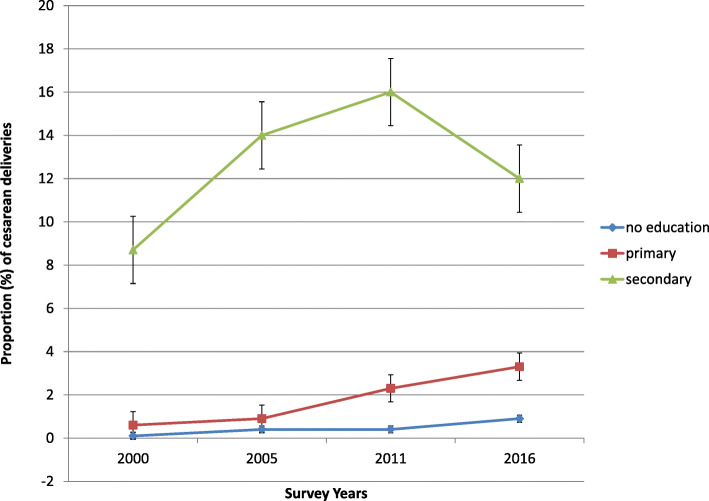
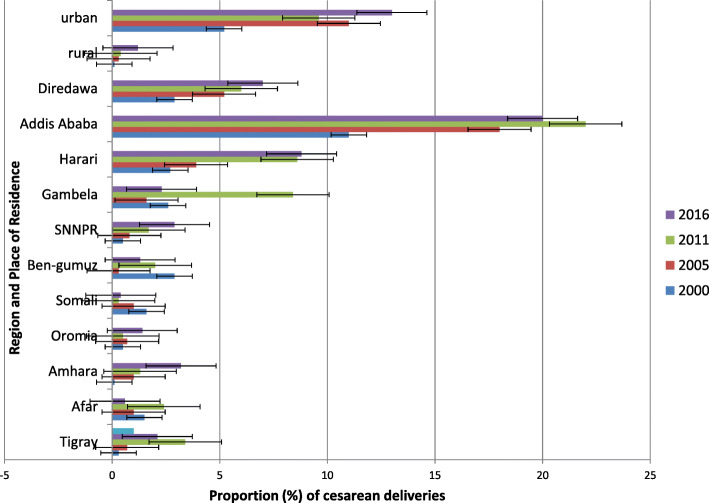
We found large socioeconomic and area-based inequalities in use of caesarean section in all study surveys. The inequalities have occurred in favour of socioeconomically advantaged women and those living in urban areas and certain regions such as Addis Ababa. While area-related inequality had generally increased with time, socioeconomic inequality showed fluctuation. Adoption of different measures in the study for the inequality analysis has caused the emergence of mix of patterns in caesarean section inequality over time.
In all the surveys, wealthy and more educated women, and those residing in urban areas had higher chance of obtaining caesarean delivery. Policy makers should work to ensure caesarean section that is in the accepted normal range. More emphasis should be drawn to subpopulation with under use of caesarean section while at the same time, discouraging unjustified use of it.
在埃塞俄比亚,使用方法严谨且成熟的方法研究剖宫产术的不平等现象的研究很少。在这项研究中,我们展示了在埃塞俄比亚,剖宫产术不平等的程度和随时间的动态变化,采用了严格的方法。
分析数据来自于 2000 年至 2016 年期间进行的埃塞俄比亚人口与健康调查(EDHS)。我们使用世界卫生组织(WHO)的卫生公平评估工具包(HEAT)来分析数据。剖宫产术根据四个公平分层因素(教育、财富、居住地和地区)进行细分。为了从不同角度捕捉不平等现象,为每个公平分层因素计算了相对和绝对综合指标。95%置信区间用于围绕点估计值计算以衡量统计显著性。
我们发现,在所有研究调查中,剖宫产术的使用存在很大的社会经济和地区不平等。这种不平等有利于社会经济地位较高的妇女以及居住在城市地区和亚的斯亚贝巴等特定地区的妇女。虽然与地区相关的不平等总体上随时间增加,但社会经济不平等存在波动。研究中对不平等分析采用不同的措施导致了剖宫产术不平等随时间出现的混合模式。
在所有调查中,富裕和受教育程度较高的妇女以及居住在城市地区的妇女获得剖宫产术的机会更高。政策制定者应努力确保剖宫产术处于可接受的正常范围内。应更加关注剖宫产术使用率较低的亚人群,同时遏制不合理的使用。