Boatin Adeline Adwoa, Schlotheuber Anne, Betran Ana Pilar, Moller Ann-Beth, Barros Aluisio J D, Boerma Ties, Torloni Maria Regina, Victora Cesar G, Hosseinpoor Ahmad Reza
Department of Obstetrics and Gynecology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Department of Information, Evidence and Research, World Health Organization, Geneva, 1211, Switzerland.
BMJ. 2018 Jan 24;360:k55. doi: 10.1136/bmj.k55.
To provide an update on economic related inequalities in caesarean section rates within countries.
Secondary analysis of demographic and health surveys and multiple indicator cluster surveys.
72 low and middle income countries with a survey conducted between 2010 and 2014 for analysis of the latest situation of inequality, and 28 countries with a survey also conducted between 2000 and 2004 for analysis of the change in inequality over time.
Women aged 15-49 years with a live birth during the two or three years preceding the survey.
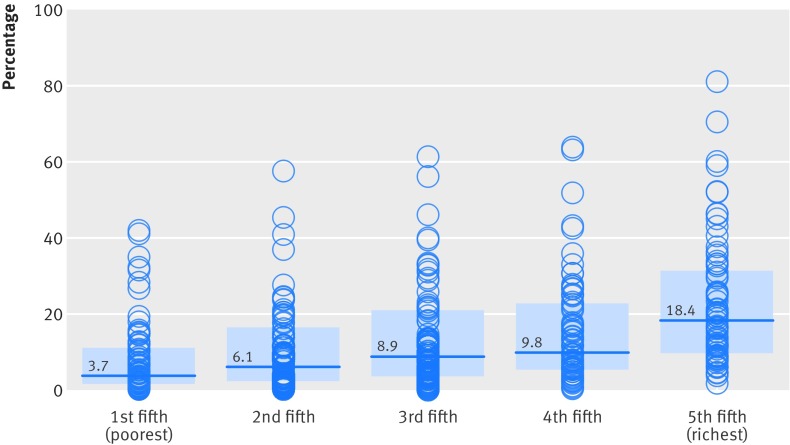
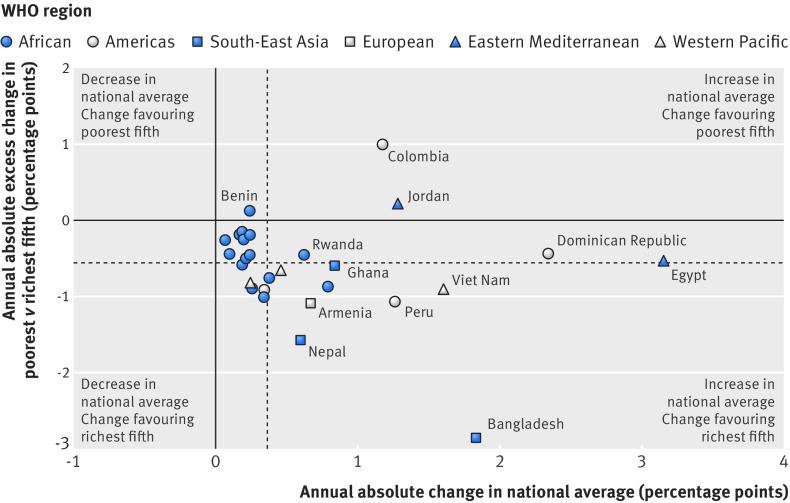
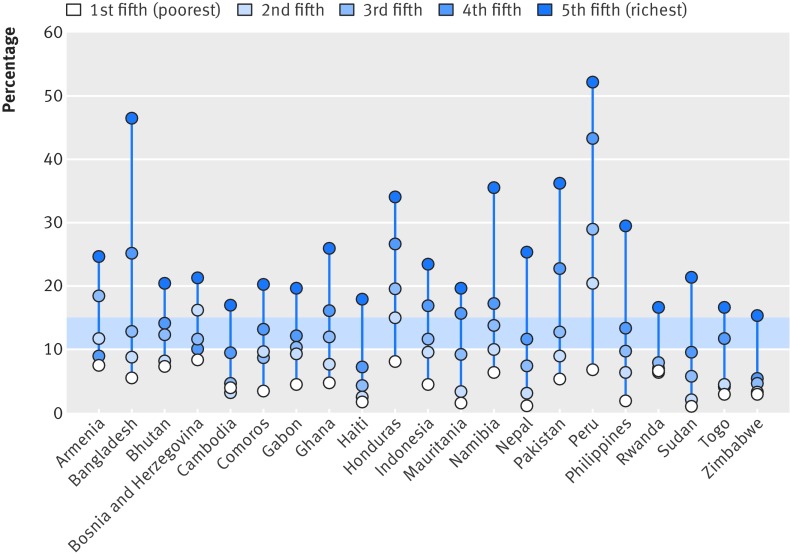
Data on caesarean section were disaggregated by asset based household wealth status and presented separately for five subgroups, ranging from the poorest to the richest fifth. Absolute and relative inequalities were measured using difference and ratio measures. The pace of change in the poorest and richest fifths was compared using a measure of excess change.
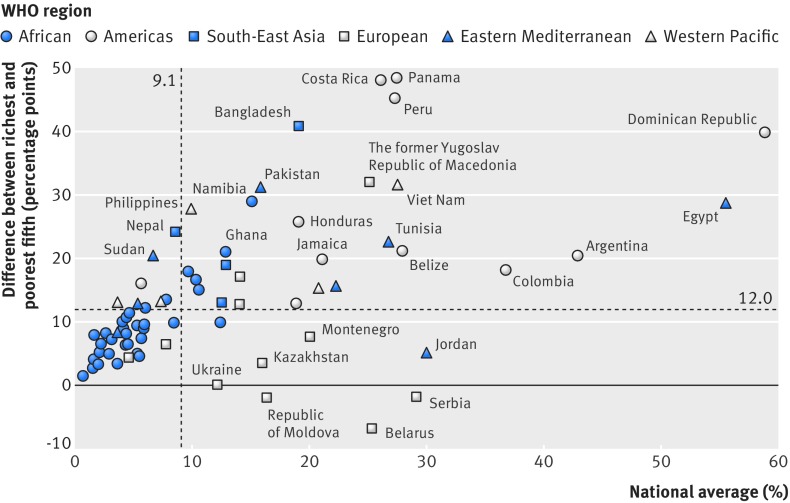
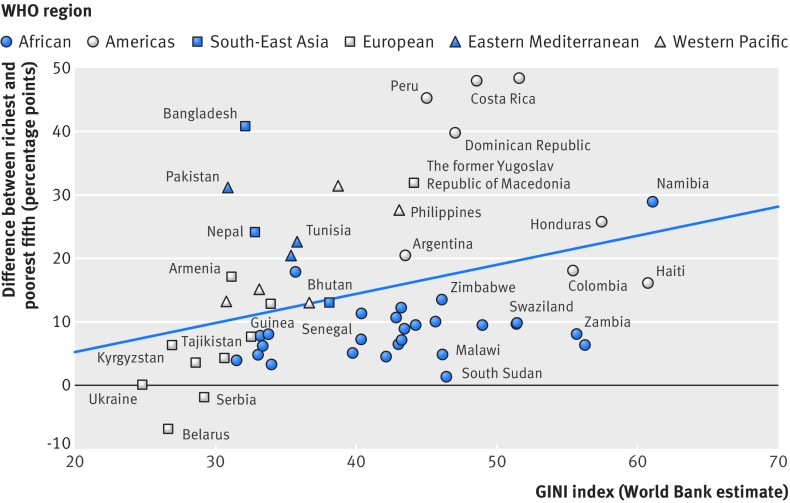
National caesarean section rates ranged from 0.6% in South Sudan to 58.9% in the Dominican Republic. Within countries, caesarean section rates were lowest in the poorest fifth (median 3.7%) and highest in the richest fifth (median 18.4%). 18 out of 72 study countries reported a difference of 20 percentage points or higher between the richest and poorest fifth. The highest caesarean section rates and greatest levels of absolute inequality were observed in countries from the region of the Americas, whereas countries from the African region had low levels of caesarean use and comparatively lower levels of absolute inequality, although relative inequality was quite high in some countries. 26 out of 28 countries reported increases in caesarean section rates over time. Rates tended to increase faster in the richest fifth (median 0.9 percentage points per year) compared with the poorest fifth (median 0.2 percentage points per year), indicating an increase in inequality over time in most of these countries.
Substantial within country economic inequalities in caesarean deliveries remain. These inequalities might be due to a combination of inadequate access to emergency obstetric care among the poorest subgroups and high levels of caesarean use without medical indication in the richest subgroups, especially in middle income countries. Country specific strategies should address these inequalities to improve maternal and newborn health.
提供各国剖宫产率方面与经济相关的不平等情况的最新信息。
对人口与健康调查以及多指标类集调查进行二次分析。
72个低收入和中等收入国家在2010年至2014年期间进行了调查以分析不平等的最新情况,28个国家在2000年至2004年期间也进行了调查以分析不平等情况随时间的变化。
在调查前两到三年有活产的15至49岁女性。
剖宫产数据按基于资产的家庭财富状况进行分类,并分别呈现给五个亚组,从最贫困的五分之一到最富有的五分之一。使用差值和比率指标来衡量绝对和相对不平等。使用超额变化指标比较最贫困和最富有的五分之一人群的变化速度。
各国剖宫产率从南苏丹的0.6%到多米尼加共和国的58.9%不等。在各国国内,剖宫产率在最贫困的五分之一人群中最低(中位数为3.7%),在最富有的五分之一人群中最高(中位数为18.4%)。72个研究国家中有18个报告最富有和最贫困的五分之一人群之间的差异为20个百分点或更高。美洲地区国家的剖宫产率最高且绝对不平等程度最大,而非洲地区国家的剖宫产使用率较低且绝对不平等程度相对较低,尽管一些国家的相对不平等程度相当高。28个国家中有26个报告剖宫产率随时间上升。与最贫困的五分之一人群(中位数为每年0.2个百分点)相比,最富有的五分之一人群的剖宫产率上升趋势更快(中位数为每年0.9个百分点),这表明在这些国家中的大多数,不平等情况随时间增加。
国内剖宫产分娩方面仍然存在显著的经济不平等。这些不平等可能是由于最贫困亚组中获得紧急产科护理的机会不足与最富有亚组中无医学指征的高剖宫产使用率共同导致的,尤其是在中等收入国家。各国应制定具体策略来解决这些不平等问题,以改善孕产妇和新生儿健康。