Højlund Mikkel, Lund Lars Christian, Herping Jonas Leander Emming, Haastrup Maija Bruun, Damkier Per, Henriksen Daniel Pilsgaard
Clinical Pharmacology and Pharmacy, Department of Public Health, University of Southern Denmark, Odense, Denmark
Department of Psychiatry Aabenraa, Mental Health Services in the Region of Southern Denmark, Aabenraa, Denmark.
BMJ Open. 2020 Aug 11;10(8):e038247. doi: 10.1136/bmjopen-2020-038247.
To examine the association between use of second-generation antipsychotics (SGA) and the risk of chronic kidney disease (CKD).
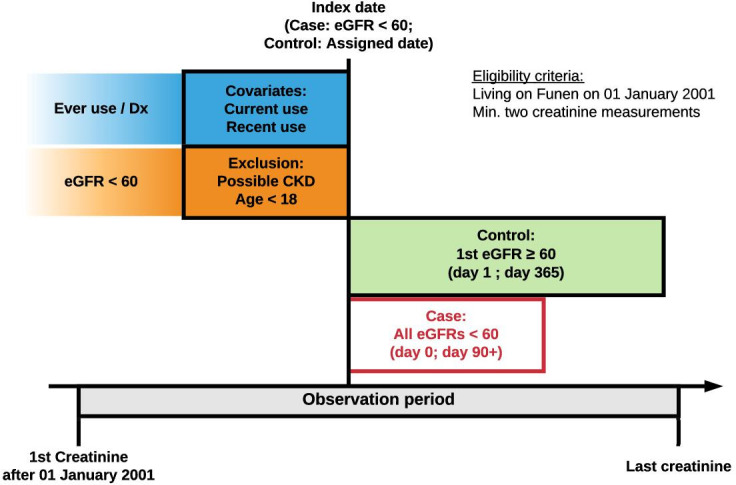
Population-based case-control study.
Routinely collected laboratory, prescription and diagnostic information on all inhabitants with creatinine measurements residing on the island of Funen, Denmark (2001 to 2015).
21 434 cases with incident CKD matched with 85 576 CKD-free population controls by risk-set sampling using age, sex and calendar year.
CKD was defined as an estimated glomerular filtration rate below 60 mL/min/1.73 m in a period longer than 3 months. Information on drug exposure and comorbidities were obtained from the Danish National Prescription Register and the Danish National Patient Register. We calculated OR for the association between SGA use and CKD using conditional logistic regression.
Use of SGAs was associated with increased risk of CKD among ever users (OR 1.24, 95% CI: 1.12 to 1.37) and current users (OR 1.26, 95% CI: 1.12 to 1.42). We found no clear evidence of dose-response relationship. Both short duration (one to two antipsychotic prescriptions; OR 1.22, 95% CI: 1.01 to 1.48) as well as long-term use (>30 prescriptions; OR 1.45, 95% CI 1.19 to 1.76) were associated with an increased risk of CKD. Both use of SGAs with mild and high risk of metabolic disturbances was associated with increased risk of CKD (OR 1.21, 95% CI: 1.06 to 1.39 and OR 1.36, 95% CI: 1.11 to 1.68, respectively). Recent use of non-steroidal anti-inflammatory drugs, prior use of lithium, hypertension or prior acute kidney injury were not clearly associated with development of CKD connected to SGA exposure. The highest risk of CKD was found for clozapine (OR 1.81, 95% CI: 1.22 to 2.69).
Use of SGA is associated with a small-to-moderately increased risk of incident CKD. All investigated SGAs, except for aripiprazole, were associated with an increased risk of CKD.
研究使用第二代抗精神病药物(SGA)与慢性肾脏病(CKD)风险之间的关联。
基于人群的病例对照研究。
对丹麦菲英岛(2001年至2015年)所有有肌酐测量值的居民的实验室、处方和诊断信息进行常规收集。
通过风险集抽样,以年龄、性别和日历年份匹配,选取21434例新发CKD病例和85576例无CKD的人群对照。
CKD定义为估计肾小球滤过率低于60 mL/min/1.73 m²且持续时间超过3个月。药物暴露和合并症信息来自丹麦国家处方登记册和丹麦国家患者登记册。我们使用条件逻辑回归计算SGA使用与CKD之间关联的比值比(OR)。
在曾经使用过SGA的人群中,使用SGA与CKD风险增加相关(OR 1.24,95%可信区间:1.12至1.37),在当前使用者中也是如此(OR 1.26,95%可信区间:1.12至1.42)。我们未发现明确的剂量反应关系证据。短期使用(一至两份抗精神病药物处方;OR 1.22,95%可信区间:1.01至1.48)以及长期使用(>30份处方;OR 1.45,95%可信区间1.19至1.76)均与CKD风险增加相关。使用具有轻度和高代谢紊乱风险的SGA均与CKD风险增加相关(分别为OR 1.21,95%可信区间:1.06至1.39和OR 1.36,95%可信区间:1.11至1.68)。近期使用非甾体抗炎药、既往使用锂盐、高血压或既往急性肾损伤与SGA暴露相关的CKD发生无明显关联。氯氮平的CKD风险最高(OR 1.81,95%可信区间:1.22至2.69)。
使用SGA与新发CKD风险有小到中度增加相关。除阿立哌唑外,所有研究的SGA均与CKD风险增加相关。