Maugars Yves, Guillot Pascale, Glémarec Joëlle, Berthelot Jean-Marie, Le Goff Benoit, Darrieutort-Laffite Christelle
Rheumatology Department, Nantes University Hospital, 1 place Alexis Ricordeau, 44093, Nantes, Cedex, France.
J Med Case Rep. 2020 Aug 11;14(1):130. doi: 10.1186/s13256-020-02401-0.
The rebound effect after stopping treatment with denosumab may be associated with rapid loss of the gains in bone mineral density achieved with treatment, high levels of bone remodeling markers, the occurrence of vertebral fractures, and even hypercalcemia.
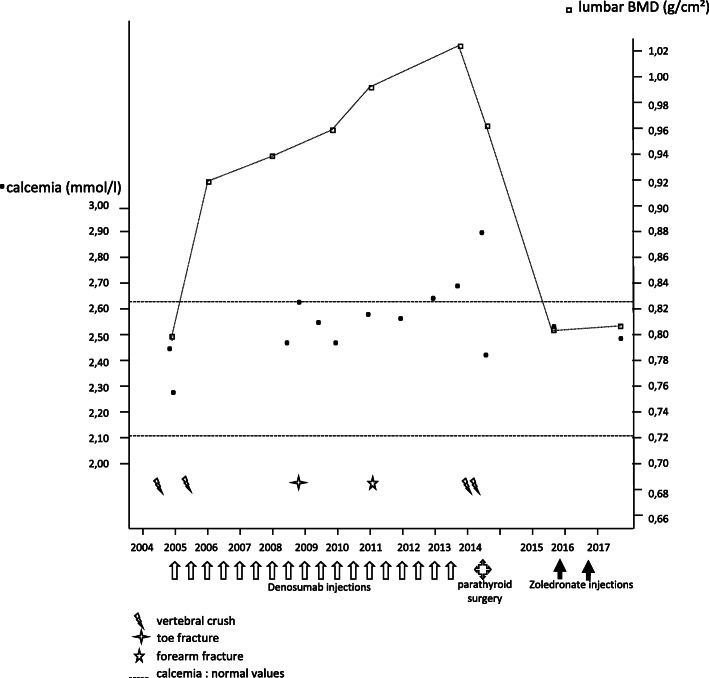
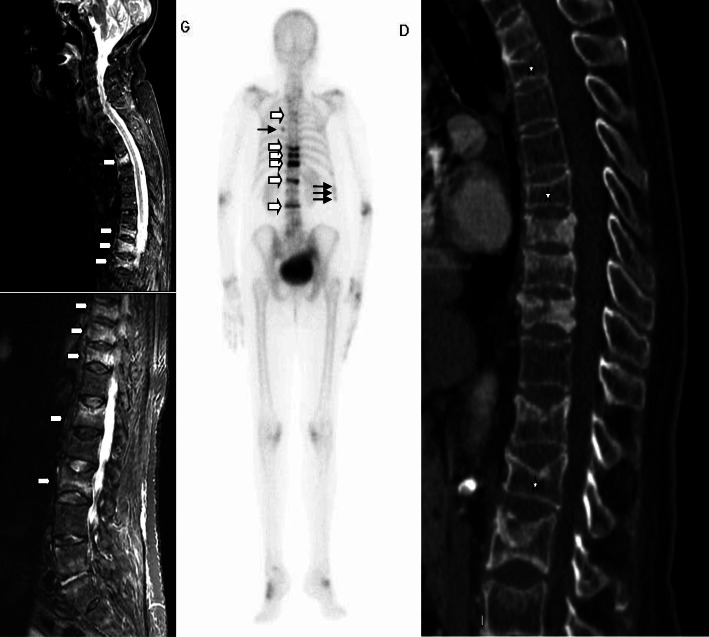
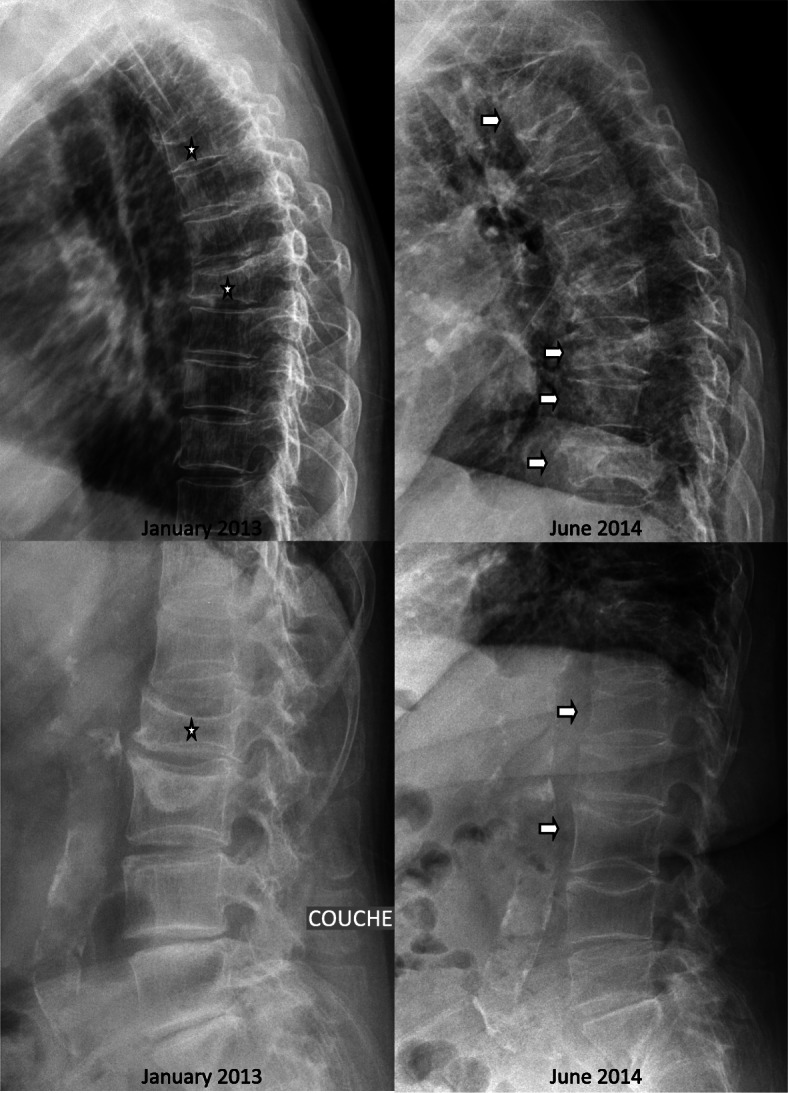
A 64-year-old osteoporotic Caucasian woman suffered from a fracture of her second lumbar vertebra in 2004. From January 2005, she was treated with denosumab for 9 years, with good densitometry results for her hip and lumbar areas, and no fractures over the last 6 years of treatment. Ten months after the treatment with denosumab was stopped, a cascade of vertebral fractures, including some in unusual locations (third thoracic vertebra), and multiple rib fractures in a context of hypercalcemia, suggested possible malignancy. A complete evaluation, including systemic, biological, and biopsy analyses, ruled out this hypothesis. The hypercalcemia was associated with normal plasma phosphate and vitamin D concentrations, and a high parathyroid hormone level, with an abnormal fixation of the lower lobe of the thyroid on sesta-methoxy-isobutyl-isonitrile scintigraphy. Histological analysis of the excised parathyroid tissue revealed hyperplasia. The associated thyroidectomy (goiter) led to the discovery of a thyroid papillary microcarcinoma.
We consider the consequences of this rebound effect, not only in terms of the major loss of bone density (return to basal values within 3 years) and the multiple disabling fracture episodes, but also in terms of the hypercalcemia observed in association with apparently autonomous tertiary hyperparathyroidism. Several cases of spontaneous reversion have been reported in children, but the intervention in our patient precluded any assessment of the possible natural course. The discovery of an associated thyroid neoplasm appears to be fortuitous. Better understanding of the various presentations of the rebound effect after stopping treatment with denosumab would improve diagnostic management of misleading forms, as in this case. Bisphosphonates could partially prevent this rebound effect.
停用地诺单抗治疗后的反跳效应可能与治疗期间所获得的骨矿物质密度快速丧失、骨重塑标志物水平升高、椎体骨折的发生,甚至高钙血症有关。
一名64岁的白种骨质疏松女性在2004年发生了第二腰椎骨折。从2005年1月起,她接受了9年的地诺单抗治疗,髋部和腰椎区域的骨密度测量结果良好,在治疗的最后6年未发生骨折。停用 地诺单抗治疗10个月后,一系列椎体骨折,包括一些发生在不寻常部位(第三胸椎)的骨折,以及在高钙血症背景下的多根肋骨骨折,提示可能为恶性肿瘤。包括全身、生物学和活检分析在内的全面评估排除了这一假设。高钙血症与血浆磷酸盐和维生素D浓度正常、甲状旁腺激素水平升高有关,在甲氧基异丁基异腈闪烁扫描中甲状腺下叶固定异常。切除的甲状旁腺组织的组织学分析显示增生。相关的甲状腺切除术(甲状腺肿)导致发现了甲状腺微小乳头状癌。
我们考虑了这种反跳效应的后果,不仅涉及骨密度的大量丧失(3年内恢复到基础值)和多次致残性骨折事件,还涉及与明显自主性三发性甲状旁腺功能亢进相关联的高钙血症。儿童中已有几例自发恢复的报道,但我们患者的干预措施排除了对可能自然病程的任何评估。相关甲状腺肿瘤的发现似乎是偶然的。更好地了解停用 地诺单抗治疗后的反跳效应的各种表现,将改善此类误导性病例的诊断管理。双膦酸盐可以部分预防这种反跳效应。