Karmanos Cancer Institute, Wayne State University School of Medicine, Detroit, Michigan, USA.
Barrow Neurological Institute, St. Joseph's Hospital & Medical Center, Phoenix, Arizona, USA.
Clin Pharmacol Ther. 2021 Feb;109(2):494-506. doi: 10.1002/cpt.2021. Epub 2020 Sep 14.
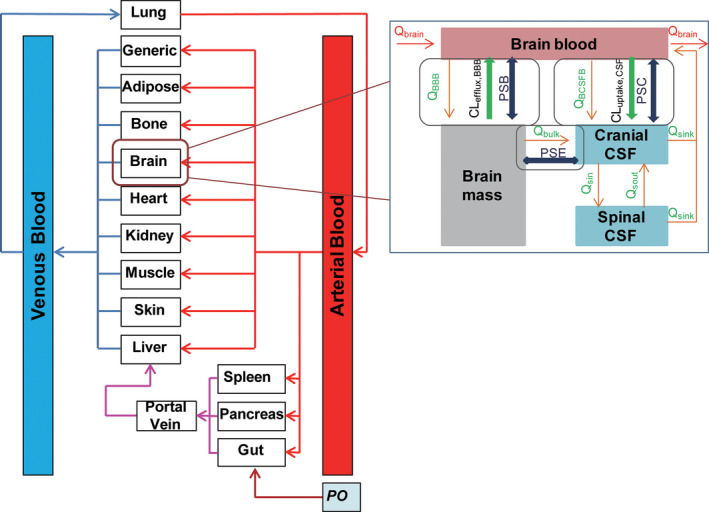
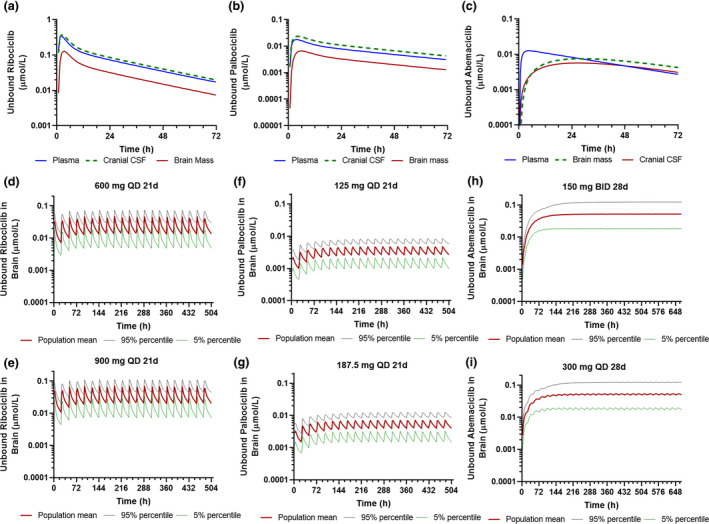
A better understanding of the human central nervous system (CNS) pharmacokinetics is critical to the selection of the right drug and refinement of dosing regimen for more effective treatment of primary and metastatic brain cancer. Using the physiologically-based pharmacokinetic (PBPK) modeling approach, we systematically compared the CNS pharmacokinetics of three cyclin D-cyclin dependent kinase 4 and 6 (CDK4/6) inhibitors (ribociclib, palbociclib, and abemaciclib) in patients with cancer. A PBPK model platform was developed and verified for predicting plasma and CNS pharmacokinetics. Target engagement ratio (TER), defined as the ratio of the average steady-state unbound drug brain concentration to the in vitro half-maximal inhibitory concentration (IC ) for CDK4/6 inhibition, was used as a crude predictor of efficacy. As compared with ribociclib and palbociclib, abemaciclib penetrated into the human brain to a larger extent, but at a slower rate, and was retained in the brain longer. Following the standard dosing regimens, the predicted CDK4/6 TERs were 26/5.2 for abemaciclib, 2.4/0.62 for ribociclib, and 0.36/0.27 for palbociclib. Simulations suggested that abemaciclib achieved comparable TERs following twice daily or daily dosing; ribociclib may sufficiently inhibit both CDK4 and CDK6 at the maximum tolerated dose; whereas, palbociclib achieved TERs < 0.5 even at a dose 50% higher than the standard dose. In conclusion, the PBPK modeling, supported by available preclinical and clinical evidence, suggests that abemaciclib is the best CDK4/6 inhibitor for brain cancer treatment, whereas palbociclib is not recommended. The model refined dosing regimen is 300 mg daily on a 4-weeks-on schedule for abemaciclib, and 900 mg daily on a 3-weeks-on/1-week-off schedule for ribociclib.
更好地了解人类中枢神经系统(CNS)的药代动力学对于选择合适的药物以及优化剂量方案以更有效地治疗原发性和转移性脑癌至关重要。使用基于生理学的药代动力学(PBPK)建模方法,我们系统地比较了三种细胞周期蛋白依赖性激酶 4 和 6(CDK4/6)抑制剂(瑞博西利、哌柏西利和阿贝西利)在癌症患者中的中枢神经系统药代动力学。开发了一个 PBPK 模型平台来预测血浆和中枢神经系统的药代动力学。靶标占有率(TER)定义为平均稳态下未结合药物脑浓度与 CDK4/6 抑制的体外半数最大抑制浓度(IC)的比值,被用作疗效的粗略预测指标。与瑞博西利和哌柏西利相比,阿贝西利更深入地渗透到人脑,但速度较慢,并且在大脑中保留的时间更长。按照标准剂量方案,预测的 CDK4/6 TER 分别为阿贝西利 26/5.2、瑞博西利 2.4/0.62 和哌柏西利 0.36/0.27。模拟表明,阿贝西利每日两次或每日给药时可达到可比的 TER;瑞博西利在最大耐受剂量下可能足以抑制 CDK4 和 CDK6;而哌柏西利即使在比标准剂量高 50%的剂量下,也无法达到 TER < 0.5。总之,PBPK 建模得到了临床前和临床证据的支持,表明阿贝西利是治疗脑癌的最佳 CDK4/6 抑制剂,而哌柏西利则不建议使用。该模型优化了剂量方案,阿贝西利的推荐剂量为每日 300mg,每 4 周为一个疗程;瑞博西利的推荐剂量为每日 900mg,每 3 周为一个疗程,然后停药 1 周。