Chatain Nicolas, Koschmieder Steffen, Jost Edgar
Department of Hematology, Oncology, Hemostaseology and Stem Cell Transplantation, Faculty of Medicine, RWTH Aachen University, 52074 Aachen, Germany.
Cancers (Basel). 2020 Aug 12;12(8):2250. doi: 10.3390/cancers12082250.
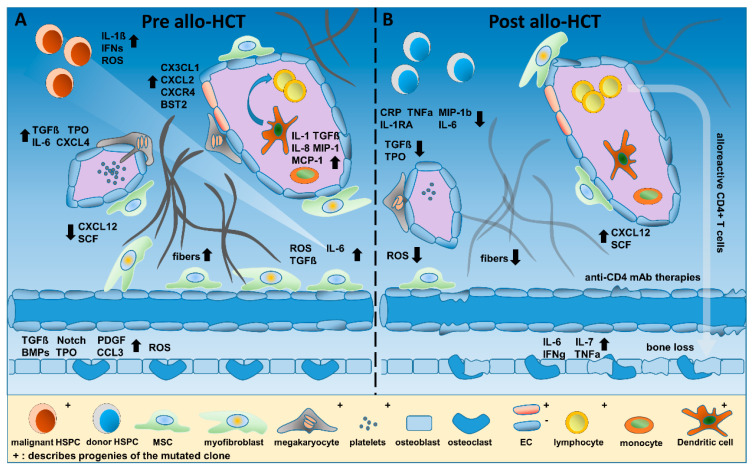
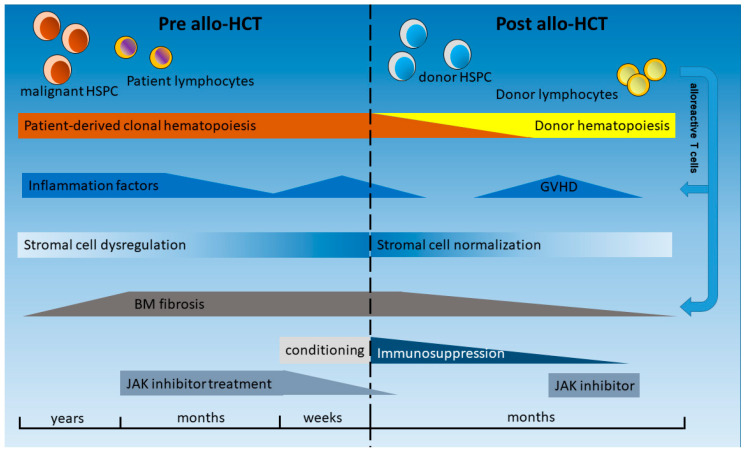
Hematopoiesis is a highly regulated and complex process involving hematopoietic stem cells (HSCs), cell surface adhesion molecules, and cytokines as well as cells of the hematopoietic niche in the bone marrow (BM). Myeloproliferative neoplasms (MPNs) are characterized by clonal expansion of HSCs involving one or more blood cell lineages. Philadelphia-negative MPNs (Ph-neg MPNs) comprise polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF). In nearly all patients with Ph-neg MPN, mutations in the genes encoding janus kinase 2 (JAK2), calreticulin (CALR), or the thrombopoietin receptor (MPL) can be detected and, together with additional mutations in epigenetic modifier genes, these genetic aberrations contribute to the clonal expansion of the cells. In addition to these intracellular changes in the malignant clone, inflammatory processes involving both the clonal and the non-clonal cells contribute to the signs and symptoms of the patients, as well as to progression of the disease to myelofibrosis (MF) or acute leukemia, and to thrombotic complications. This contribution has been corroborated in preclinical studies including mouse models and patient-derived iPS cells, and in clinical trials, using anti-inflammatory drugs such as JAK inhibitors and steroids, or immunomodulatory drugs such as IMiDs and interferon-alpha (IFNa), all of which change the (im)balance of circulating inflammatory factors (e.g., TNFa, IL-1b, and TGFβ) in MPN. Currently, allogeneic hematopoietic (stem) cell transplantation (allo-HCT) remains the only curative treatment for Ph-neg MPN and is the treatment of choice in intermediate-2 and high-risk MF. HCT can reverse inflammatory changes induced by MPN as well as fibrosis in a large proportion of patients, but it also induces itself profound changes in inflammatory cells and cytokines in the patient, which may help to eradicate the disease but also in part cause significant morbidity (e.g., by graft-versus-host disease). In this review, we focus on the contribution of aberrant inflammation to disease pathogenesis in Ph-neg MPN as well as the current understanding of its alterations after allogeneic HCT.
造血是一个高度调控且复杂的过程,涉及造血干细胞(HSC)、细胞表面黏附分子、细胞因子以及骨髓(BM)中造血微环境的细胞。骨髓增殖性肿瘤(MPN)的特征是造血干细胞的克隆性扩增,涉及一种或多种血细胞谱系。费城阴性MPN(Ph-neg MPN)包括真性红细胞增多症(PV)、原发性血小板增多症(ET)和原发性骨髓纤维化(PMF)。在几乎所有Ph-neg MPN患者中,均可检测到编码Janus激酶2(JAK2)、钙网蛋白(CALR)或血小板生成素受体(MPL)的基因突变,并且这些遗传异常与表观遗传修饰基因中的其他突变一起,促成了细胞的克隆性扩增。除了恶性克隆中的这些细胞内变化外,涉及克隆细胞和非克隆细胞的炎症过程也导致了患者的体征和症状,以及疾病进展为骨髓纤维化(MF)或急性白血病,还有血栓形成并发症。在包括小鼠模型和患者来源的诱导多能干细胞(iPS细胞)的临床前研究以及临床试验中,使用JAK抑制剂和类固醇等抗炎药物或沙利度胺类似物(IMiD)和α干扰素(IFNa)等免疫调节药物,均证实了这种作用,所有这些药物都会改变MPN中循环炎症因子(如肿瘤坏死因子α、白细胞介素-1β和转化生长因子β)的(失衡)平衡。目前,异基因造血(干细胞)细胞移植(allo-HCT)仍然是Ph-neg MPN的唯一治愈性治疗方法,并且是中-2和高危MF的首选治疗方法。HCT可以在很大一部分患者中逆转MPN诱导的炎症变化以及纤维化,但它本身也会在患者体内引起炎症细胞和细胞因子的深刻变化,这可能有助于根除疾病,但也部分地导致显著的发病率(例如通过移植物抗宿主病)。在这篇综述中,我们关注异常炎症对Ph-neg MPN疾病发病机制的作用以及目前对异基因HCT后其变化的理解。