Department of Urology, Comprehensive Cancer Center, Vienna General Hospital Medical University of Vienna, Währinger Gürtel 18-20, 1090, Vienna, Austria.
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia.
World J Urol. 2021 Jun;39(6):1961-1968. doi: 10.1007/s00345-020-03384-9. Epub 2020 Aug 17.
The De Ritis ratio (aspartate aminotransferase/alanine aminotransferase, DRR) has been linked to oncological outcomes in several cancers. We aimed to assess the association of DRR with recurrence-free survival (RFS) and progression-free survival (PFS) in patients with non-muscle-invasive bladder cancer (NMIBC).
We conducted a retrospective analysis of 1117 patients diagnosed with NMIBC originating from an established multicenter database. To define the optimal pretreatment DRR cut-off value, we determined a value of 1.2 as having a maximum Youden index value. The overall population was therefore divided into two De Ritis ratio groups using this cut-off (lower, < 1.2 vs. higher, ≥ 1.2). Univariable and multivariable Cox regression analyses were used to investigate the association of DRR with RFS and PFS. The discrimination of the model was evaluated with the Harrel's concordance index (C-index).
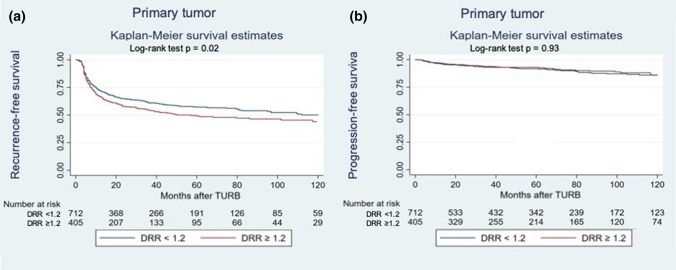
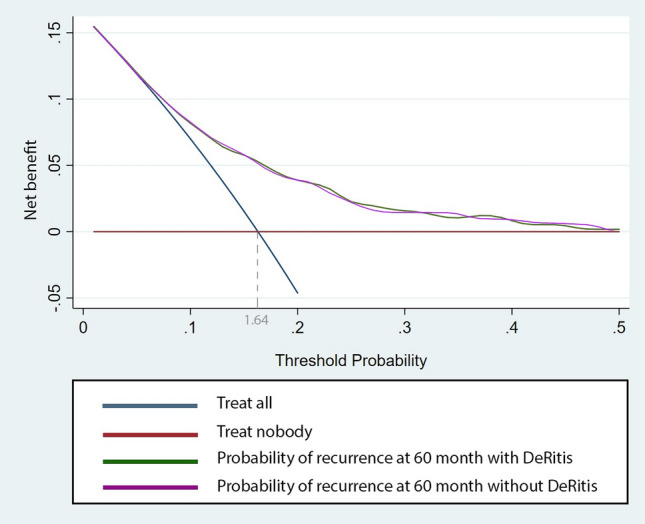
Overall, 405 (36%) patients had a DRR ≥ 1.2. On univariable Cox regression analysis, DRR was significantly associated with RFS (HR: 1.23, 95% CI 1.02-1.47, p = 0.03), but not with PFS (HR: 0.96, 95% CI 0.65-1.44, p = 0.9). On multivariable Cox regression analysis, which adjusted for the effect of established clinicopathologic features, DRR ≥ 1.2 remained significantly associated with worse RFS (HR:1.21, 95% CI 1.00-1.46, p = 0.04). The addition of DRR only minimally improved the discrimination of a base model that included established clinicopathologic features (C-index = 0.683 vs. C-index = 0.681). On DCA the inclusion of DRR did not improve the net-benefit of the prognostic model.
Despite the statistically significant association of the DRR with RFS in patients with NMIBC, it does not seem to add any prognostic or clinical benefit beyond that of currently available clinical factors.
天门冬氨酸氨基转移酶/丙氨酸氨基转移酶(DRR)比值与多种癌症的肿瘤学结局相关。我们旨在评估其与非肌层浸润性膀胱癌(NMIBC)患者无复发生存率(RFS)和无进展生存率(PFS)的相关性。
我们对源自一个既定多中心数据库的 1117 例 NMIBC 患者进行了回顾性分析。为了确定最佳的预处理 DRR 截断值,我们确定了 1.2 作为具有最大 Youden 指数值的数值。因此,总体人群根据该截断值(低值,<1.2 与高值,≥1.2)分为两个 DRR 比值组。使用单变量和多变量 Cox 回归分析来研究 DRR 与 RFS 和 PFS 的相关性。使用 Harrell 的一致性指数(C-index)评估模型的区分能力。
总体而言,405(36%)例患者的 DRR≥1.2。在单变量 Cox 回归分析中,DRR 与 RFS 显著相关(HR:1.23,95%CI 1.02-1.47,p=0.03),但与 PFS 无关(HR:0.96,95%CI 0.65-1.44,p=0.9)。在多变量 Cox 回归分析中,调整了既定临床病理特征的影响后,DRR≥1.2 仍与 RFS 较差显著相关(HR:1.21,95%CI 1.00-1.46,p=0.04)。仅增加 DRR 仅略微提高了包含既定临床病理特征的基础模型的区分能力(C-index=0.683 与 C-index=0.681)。在 DCA 中,纳入 DRR 并未改善预后模型的净收益。
尽管 DRR 与 NMIBC 患者的 RFS 呈统计学显著相关,但它似乎并没有在目前可用的临床因素之外提供任何预后或临床获益。