Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Department of Urology, King Fahad Specialist Hospital, Dammam, Saudi Arabia.
World J Urol. 2021 Sep;39(9):3345-3352. doi: 10.1007/s00345-020-03586-1. Epub 2021 Jan 26.
To investigate the prognostic value of preoperative serum albumin to globulin ratio (AGR) in patients with non-muscle-invasive bladder cancer (NMIBC) treated with transurethral resection of bladder tumor (TURB) with or without intravesical therapy (IVT).
We retrospectively reviewed 1,096 consecutive patients with NMIBC. Levels of albumin and globulin were obtained before TURB and used to calculate the preoperative AGR level. Multivariable Cox regression analyses were performed to assess the prognostic effect of preoperative AGR on oncologic outcomes. Subgroup analyses were performed in patients based on the European Association of Urology (EAU) risk groups for NMIBC.
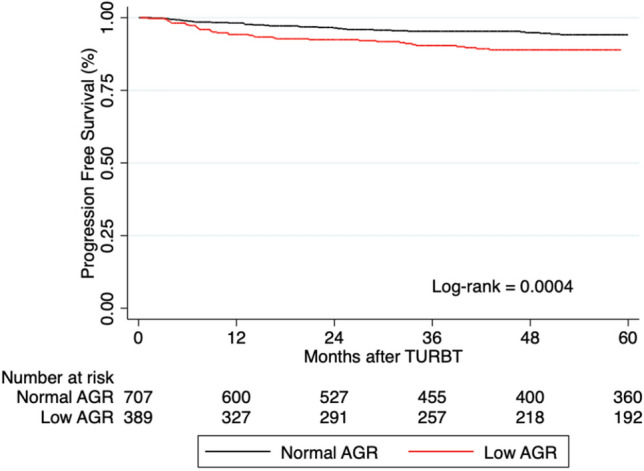
Low AGR levels were observed in 389 (35.5%) patients. The median follow-up was 63.7 months (IQR 25.3-111). On multivariable Cox regression analysis, low AGR was associated with increased risk of progression to muscle-invasive BCa (MIBC) (HR 1.81, 95% CI 1.22-2.68, P = 0.003). The addition of AGR only minimally improved the discrimination ability of a base model that included established clinicopathologic features (C-index = 0.7354 vs. C-index = 0.7162). Low preoperative AGR was not significantly associated with the risk of disease recurrence (P = 0.31). In subgroup analyses based on patients' EAU risk groups, low preoperative AGR was not associated with recurrence-free survival (RFS) (P = 0.59) or progression-free survival (PFS) (P = 0.22) in any of the risk groups. Additionally, in patients treated with Bacillus Calmette-Guerin (BCG) for intermediate- or high-risk NMIBC, low AGR failed to predict disease recurrence or progression.
Preoperative serum AGR levels independently predicted the risk of disease progression in patients with NMIBC. However, it was not found to be associated with either RFS or PFS in NMIBC patients based on their EAU risk group. This marker seems to have a limited role in NMIBC at the present time. However, further research is needed to investigate this marker in combination with other systemic inflammatory markers to help improve prediction in this heterogeneous group of patients.
研究术前血清白蛋白/球蛋白比值(AGR)在接受经尿道膀胱肿瘤切除术(TURB)联合或不联合膀胱内治疗(IVT)的非肌层浸润性膀胱癌(NMIBC)患者中的预后价值。
我们回顾性分析了 1096 例连续的 NMIBC 患者。在 TURB 前获得白蛋白和球蛋白水平,并用于计算术前 AGR 水平。采用多变量 Cox 回归分析评估术前 AGR 对肿瘤学结局的预后影响。根据欧洲泌尿外科学会(EAU)NMIBC 风险分组对患者进行亚组分析。
389 例(35.5%)患者的 AGR 水平较低。中位随访时间为 63.7 个月(IQR 25.3-111)。多变量 Cox 回归分析显示,低 AGR 与向肌层浸润性膀胱癌(MIBC)进展的风险增加相关(HR 1.81,95%CI 1.22-2.68,P=0.003)。AGR 的加入仅略微提高了包括既定临床病理特征的基础模型的区分能力(C 指数=0.7354 与 C 指数=0.7162)。低术前 AGR 与疾病复发风险无显著相关性(P=0.31)。根据患者 EAU 风险分组的亚组分析,低术前 AGR 与任何风险组的无复发生存率(RFS)(P=0.59)或无进展生存率(PFS)(P=0.22)均无显著相关性。此外,在接受卡介苗(BCG)治疗中高危 NMIBC 的患者中,低 AGR 未能预测疾病复发或进展。
术前血清 AGR 水平独立预测 NMIBC 患者疾病进展的风险。然而,根据 EAU 风险组,它与 NMIBC 患者的 RFS 或 PFS 均无相关性。目前,该标志物在 NMIBC 中的作用有限。然而,需要进一步研究以探讨该标志物与其他全身炎症标志物联合应用,以帮助改善该异质患者群体的预测。