Department of Neurosurgery, Oslo University Hospital, P O Box 4950, Nydalen, 0424, Oslo, Norway.
Faculty of Medicine, Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
Acta Neurochir (Wien). 2020 Dec;162(12):3107-3116. doi: 10.1007/s00701-020-04538-9. Epub 2020 Aug 18.
Fatigue is a common and disabling sequel after aneurysmal subarachnoid hemorrhage (aSAH). At present, prevalence estimates of post-aSAH fatigue in the chronic phase are scarce and vary greatly. Factors from the acute phase of aSAH have hitherto barely been associated with post-aSAH fatigue in the chronic phase.
Prospective study assessing prevalence of fatigue using the Fatigue Severity Scale (FSS) in patients who were living independently 1 to 7 years after aSAH. We compared demographic, medical, and radiological variables from the acute phase of aSAH between patients with and without fatigue (FSS ≥ 4 versus < 4) and searched for predictors of fatigue among these variables applying univariable and multivariable regression analyses.
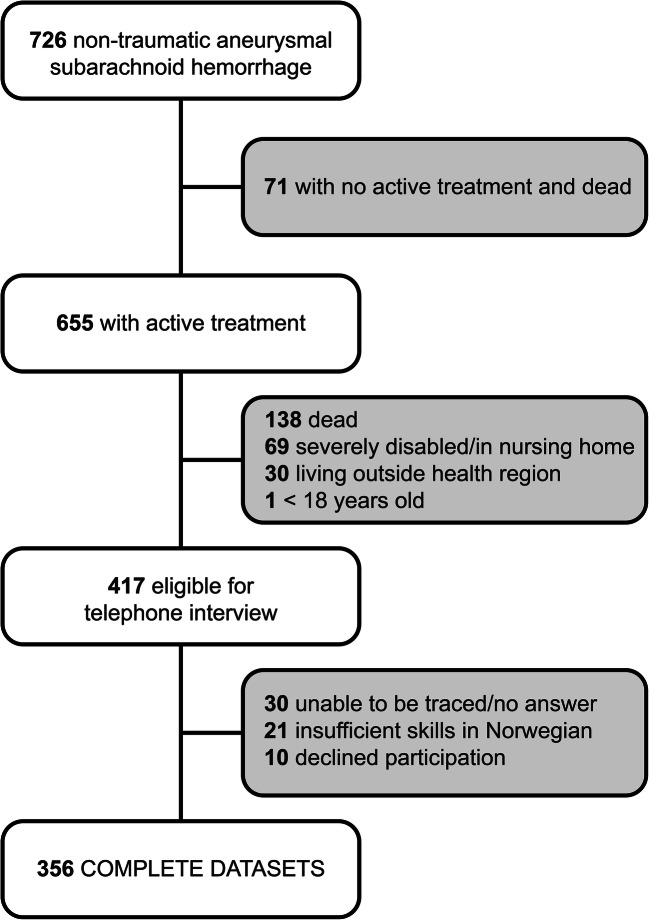
Of 726 patients treated for aSAH in the period between January 2012 and December 2017, 356 patients completed the assessment. The mean FSS score was 4.7 ± 1.7, and fatigue was present in 69.7%. The frequency of patients with fatigue did not decline significantly over time. Univariable analysis identified nicotine use, loss of consciousness at ictus (LOCi), rebleed prior to aneurysm repair, reduced consciousness to Glasgow Coma Scale (GCS) < 14, large amounts of subarachnoid blood, the presence of acute hydrocephalus, and severe vasospasm as factors that were significantly associated with fatigue. In multivariable analysis, nicotine use, reduced GCS, and severe vasospasm were independent predictors that all more than doubled the risk to develop post-aSAH fatigue.
Fatigue is a frequent sequel persisting several years after aSAH. Nicotine use, reduced consciousness at admission, and severe vasospasm are independent predictors of fatigue from the acute phase of aSAH. We propose inflammatory cytokines causing dopamine imbalance to be a common denominator for post-aSAH fatigue and the presently identified predictors.
疲劳是蛛网膜下腔出血(aSAH)后常见且致残的后遗症。目前,慢性期 aSAH 后疲劳的患病率估计很少且差异很大。迄今为止,aSAH 急性期的因素几乎与慢性期的 aSAH 后疲劳无关。
前瞻性研究使用疲劳严重程度量表(FSS)评估 aSAH 后 1 至 7 年独立生活的患者的疲劳患病率。我们比较了患有和不患有疲劳(FSS≥4 与 <4)的患者在 aSAH 急性期的人口统计学、医学和影像学变量,并在这些变量中应用单变量和多变量回归分析寻找疲劳的预测因素。
在 2012 年 1 月至 2017 年 12 月期间治疗的 726 名 aSAH 患者中,有 356 名患者完成了评估。平均 FSS 评分为 4.7±1.7,疲劳发生率为 69.7%。随着时间的推移,患有疲劳的患者频率并没有明显下降。单变量分析确定了尼古丁使用、发作时意识丧失(LOCi)、在动脉瘤修复前再出血、格拉斯哥昏迷量表(GCS)<14 的意识降低、大量蛛网膜下腔出血、急性脑积水的存在和严重血管痉挛与疲劳显著相关。多变量分析表明,尼古丁使用、GCS 降低和严重血管痉挛是独立的预测因素,所有这些因素使发生 aSAH 后疲劳的风险增加了一倍以上。
疲劳是 aSAH 后持续数年的常见后遗症。尼古丁使用、入院时意识降低和严重血管痉挛是 aSAH 急性期疲劳的独立预测因素。我们提出引起多巴胺失衡的炎症细胞因子是 aSAH 后疲劳和目前确定的预测因素的共同因素。