Health Policy, Quality and Informatics Program, Health Services Research and Development, Center for Innovations in Quality, Effectiveness, and Safety, Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas.
Section of Health Services Research, Department of Medicine, Baylor College of Medicine, Houston, Texas.
JAMA Netw Open. 2020 Aug 3;3(8):e2011051. doi: 10.1001/jamanetworkopen.2020.11051.
Studies on the use of and adherence to secondary prevention therapies in patients with premature and extremely premature atherosclerotic cardiovascular disease (ASCVD) are lacking.
To evaluate and compare aspirin use, any statin use, high-intensity statin use, and statin adherence among patients with premature or extremely premature ASCVD compared with patients with nonpremature ASCVD.
DESIGN, SETTING, AND PARTICIPANTS: This multicenter cross-sectional study used the clinical and administrative data sets of the US Department of Veterans Affairs (VA) to identify adult patients with at least 1 primary care visit in the VA health care system between October 1, 2014, and September 30, 2015. The study cohort comprised patients with ASCVD (ischemic heart disease, peripheral arterial disease, or ischemic cerebrovascular disease) who were enrolled in the Veterans With Premature Atherosclerosis (VITAL) registry. Patients with missing data for date of birth or sex and those with limited life expectancy were excluded. Data were analyzed from November 1, 2019, to January 1, 2020.
Premature (the first ASCVD event occurred at age <55 years for men and age <65 years for women) vs nonpremature (the first ASCVD event occurred at age ≥55 years for men or age ≥65 years for women) ASCVD and extremely premature (the first ASCVD event occurred at age <40 years) vs nonpremature ASCVD.
The primary outcomes were aspirin use, any statin use, high-intensity statin use, and statin adherence (measured by proportion of days covered [PDC] ≥0.8).
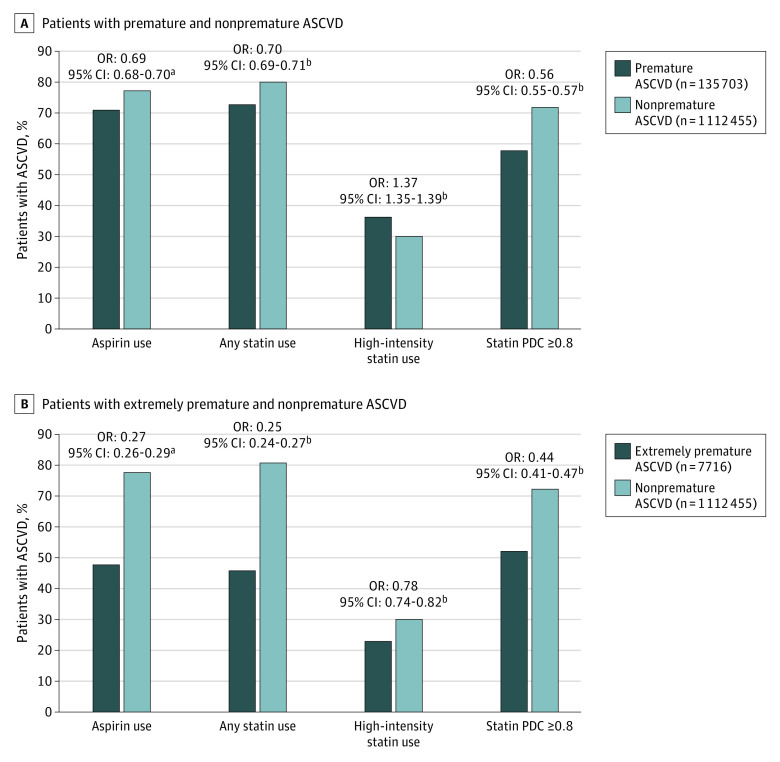
Of the 1 248 158 patients identified, 135 703 (10.9%) had premature ASCVD (mean [SD] age, 49.6 [5.8] years; 116 739 men [86.0%]), 1 112 455 (89.1%) had nonpremature ASCVD (mean [SD] age, 69.6 [8.9] years; 1 104 318 men [99.3%]), and 7716 (0.6%) had extremely premature ASCVD (mean [SD] age, 34.2 [4.3] years; 6576 men [85.2%]). Patients with premature ASCVD vs those with nonpremature ASCVD had lower rates of aspirin use (96 468 [71.1%] vs 860 726 [77.4%]; P < .001) and any statin use (98 908 [72.9%] vs 894 931 [80.5%]; P < .001); had a statin PDC of 0.8 or higher (57 306 [57.9%] vs 644 357 [72.0%]; P < .001); and a higher rate of high-intensity statin use (49 354 [36.4%] vs 332 820 [29.9%]; P < .001). Similarly, patients with extremely premature ASCVD were less likely to use aspirin (odds ratio [OR], 0.27; 95% CI, 0.26-0.29), any statin (OR, 0.25; 95% CI, 0.24-0.27), or high-intensity statin (OR, 0.78; 95% CI, 0.74-0.82) and to be statin adherent (OR, 0.44; 95% CI, 0.41-0.47).
In this study, patients with premature or extremely premature ASCVD appeared to be less likely to use aspirin or statins and to adhere to statin therapy. This finding warrants further investigation into premature ASCVD and initiatives, including clinician and patient education, to better understand and mitigate the disparities in medication use and adherence.
关于使用和坚持二级预防治疗的研究在患有早发和极早发动脉粥样硬化性心血管疾病(ASCVD)的患者中缺乏。
评估和比较早发或极早发 ASCVD 患者与非早发 ASCVD 患者相比,使用阿司匹林、任何他汀类药物、高强度他汀类药物和他汀类药物的依从性。
设计、地点和参与者:这项多中心横断面研究使用了美国退伍军人事务部(VA)的临床和行政数据集,以确定在 2014 年 10 月 1 日至 2015 年 9 月 30 日期间在 VA 医疗保健系统中至少有一次初级保健就诊的成年患者。研究队列包括患有 ASCVD(缺血性心脏病、外周动脉疾病或缺血性脑血管疾病)的患者,他们参加了退伍军人早发动脉粥样硬化(VITAL)登记处。排除了出生日期或性别缺失数据和预期寿命有限的患者。数据于 2019 年 11 月 1 日至 2020 年 1 月 1 日进行分析。
早发(首次 ASCVD 事件发生在男性年龄<55 岁或女性年龄<65 岁)与非早发(首次 ASCVD 事件发生在男性年龄≥55 岁或女性年龄≥65 岁)和极早发(首次 ASCVD 事件发生在男性年龄<40 岁或女性年龄<40 岁)与非早发 ASCVD。
主要结果是阿司匹林的使用、任何他汀类药物的使用、高强度他汀类药物的使用和他汀类药物的依从性(通过比例天数覆盖[PDC]≥0.8 来衡量)。
在确定的 1248158 名患者中,135703 名(10.9%)患有早发 ASCVD(平均[标准差]年龄 49.6[5.8]岁;116739 名男性[86.0%]),1112455 名(89.1%)患有非早发 ASCVD(平均[标准差]年龄 69.6[8.9]岁;1104318 名男性[99.3%]),7716 名(0.6%)患有极早发 ASCVD(平均[标准差]年龄 34.2[4.3]岁;6576 名男性[85.2%])。与非早发 ASCVD 患者相比,早发 ASCVD 患者阿司匹林使用率(96468[71.1%]比 860726[77.4%];P<0.001)和任何他汀类药物使用率(98908[72.9%]比 894931[80.5%];P<0.001)较低;他汀类药物 PDC 为 0.8 或更高(57306[57.9%]比 644357[72.0%];P<0.001);高强度他汀类药物使用率较高(49354[36.4%]比 332820[29.9%];P<0.001)。同样,极早发 ASCVD 患者使用阿司匹林(优势比[OR],0.27;95%置信区间[CI],0.26-0.29)、任何他汀类药物(OR,0.25;95%CI,0.24-0.27)或高强度他汀类药物(OR,0.78;95%CI,0.74-0.82)的可能性较低,他汀类药物的依从性(OR,0.44;95%CI,0.41-0.47)也较低。
在这项研究中,早发或极早发 ASCVD 患者似乎不太可能使用阿司匹林或他汀类药物,也不太可能坚持他汀类药物治疗。这一发现需要进一步研究早发 ASCVD,并采取包括临床医生和患者教育在内的举措,以更好地了解和减轻药物使用和依从性方面的差异。