Yamamoto Ryo, Yoshizawa Jo
Department of Emergency and Critical Care Medicine, Keio University School of Medicine, 35 Shinanomachi, Shinjuku, Tokyo, 160-8582 Japan.
J Intensive Care. 2020 Aug 12;8:60. doi: 10.1186/s40560-020-00477-w. eCollection 2020.
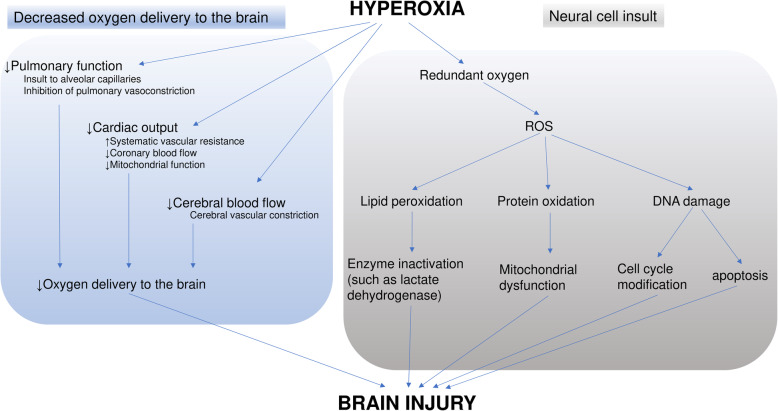
High oxygen tension in blood and/or tissue affects clinical outcomes in several diseases. Thus, the optimal target PaO for patients recovering from cardiac arrest (CA) has been extensively examined. Many patients develop hypoxic brain injury after the return of spontaneous circulation (ROSC); this supports the need for oxygen administration in patients after CA. Insufficient oxygen delivery due to decreased blood flow to cerebral tissue during CA results in hypoxic brain injury. By contrast, hyperoxia may increase dissolved oxygen in the blood and, subsequently, generate reactive oxygen species that are harmful to neuronal cells. This secondary brain injury is particularly concerning. Although several clinical studies demonstrated that hyperoxia during post-CA care was associated with poor neurological outcomes, considerable debate is ongoing because of inconsistent results. Potential reasons for the conflicting results include differences in the definition of hyperoxia, the timing of exposure to hyperoxia, and PaO values used in analyses. Despite the conflicts, exposure to PaO > 300 mmHg through administration of unnecessary oxygen should be avoided because no obvious benefit has been demonstrated. The feasibility of titrating oxygen administration by targeting SpO at approximately 94% in patients recovering from CA has been demonstrated in pilot randomized controlled trials (RCTs). Such protocols should be further examined.
血液和/或组织中的高氧张力会影响多种疾病的临床预后。因此,人们对心脏骤停(CA)复苏患者的最佳目标动脉血氧分压(PaO)进行了广泛研究。许多患者在自主循环恢复(ROSC)后会发生缺氧性脑损伤;这支持了CA后患者需要吸氧的观点。CA期间由于脑组织血流减少导致的氧输送不足会导致缺氧性脑损伤。相比之下,高氧可能会增加血液中溶解的氧,随后产生活性氧,对神经元细胞有害。这种继发性脑损伤尤其令人担忧。尽管多项临床研究表明,CA后护理期间的高氧与不良神经预后相关,但由于结果不一致,仍存在相当大的争议。结果相互矛盾的潜在原因包括高氧的定义、高氧暴露的时间以及分析中使用的PaO值存在差异。尽管存在争议,但应避免通过给予不必要的氧气使PaO>300 mmHg,因为尚未证明有明显益处。在初步随机对照试验(RCT)中已证明,对于CA复苏患者,以大约94%的脉搏血氧饱和度(SpO)为目标滴定吸氧的可行性。此类方案应进一步研究。