Cox Jennie, Ryan Patrick, Burkle Jeff, Jandarov Roman, Mendell Mark J, Hershey Gurjit Khurana, LeMasters Grace, Reponen Tiina
Department of Environmental Health, University of Cincinnati, Cincinnati, Ohio.
Division of Biostatistics and Epidemiology, Department of Pediatrics, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio.
Environ Epidemiol. 2020 Jun 19;4(4):e101. doi: 10.1097/EE9.0000000000000101. eCollection 2020 Aug.
Previous epidemiologic studies of dampness and mold relied on metrics that did not fully assess exposure-response relationships. Our objective was to examine quantitative metrics of dampness and mold during infancy and respiratory health outcomes during childhood.
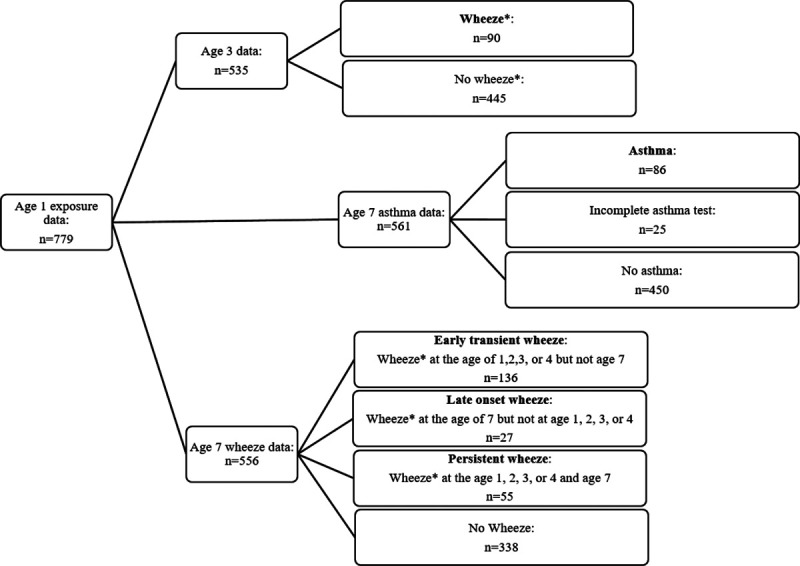
In-home visits were conducted before age 1 for children in the Cincinnati Childhood Allergy and Air Pollution Study. Respiratory outcomes included age 3 wheeze and age 7 asthma and wheeze. The associations between home exposure and respiratory outcomes were evaluated for 779 children using logistic regression adjusting for household income, neighborhood socioeconomic status, and the presence of pests.
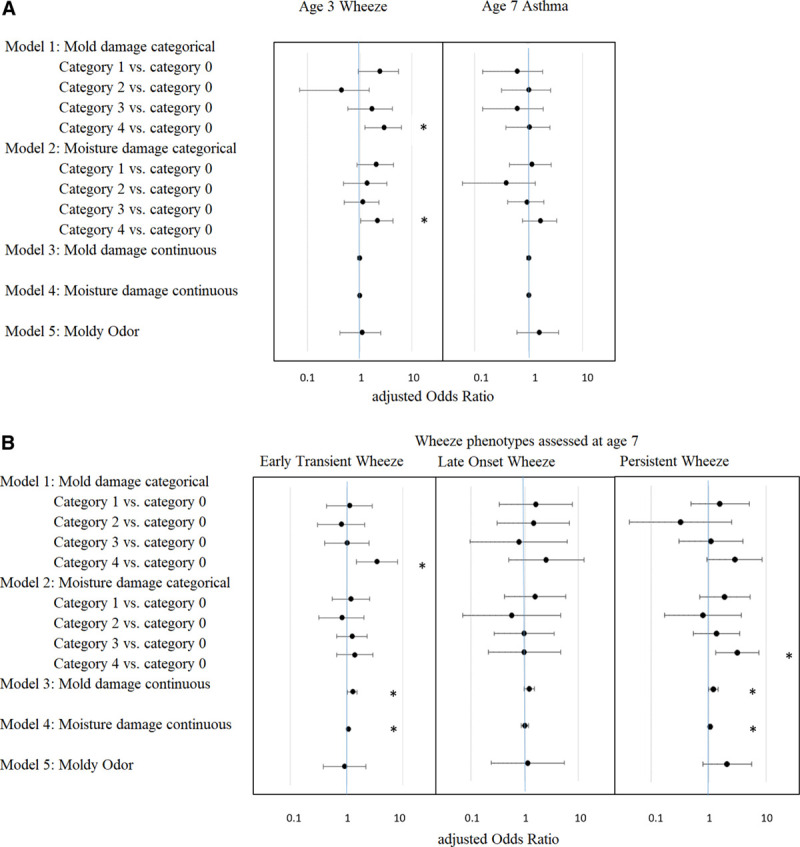
Children residing in homes with ≥0.29 m of moisture damage were significantly more likely to have wheezing at age 3 and persistent wheeze through age 7 (adjusted odds ratio [aOR] = 2.2; 95% confidence interval [CI] = 1.0, 4.3 and aOR = 3.2; CI = 1.3, 7.5, respectively). Additionally, homes having ≥0.19 m of mold damage were associated with wheezing at age 3 and early transient wheeze assessed at age 7 (aOR = 2.9; CI = 1.3, 6.4 and aOR = 3.5; CI = 1.5, 8.2, respectively). Mold damage <0.19 m and moisture damage <0.29 m were not associated with health outcomes. Mold and moisture damage were also not associated with asthma.
Our data indicate that only the highest categories analyzed for mold (≥0.19 m) and moisture damage (≥0.29 m) in homes at age 1 were significantly associated with wheeze at ages 3 and 7; however, data below these levels were too sparse to assess the shape of the relationship or explore potential health-relevant thresholds.
以往关于潮湿和霉菌的流行病学研究依赖于不能充分评估暴露-反应关系的指标。我们的目标是研究婴儿期潮湿和霉菌的定量指标以及儿童期的呼吸健康结果。
在辛辛那提儿童过敏与空气污染研究中,对1岁前的儿童进行家访。呼吸结果包括3岁时的喘息和7岁时的哮喘及喘息。使用逻辑回归评估了779名儿童家庭暴露与呼吸结果之间的关联,并对家庭收入、邻里社会经济地位和害虫存在情况进行了调整。
居住在潮湿损坏≥0.29米房屋中的儿童在3岁时喘息以及到7岁时持续喘息的可能性显著更高(调整后的优势比[aOR]=2.2;95%置信区间[CI]=1.0,4.3和aOR=3.2;CI=1.3,7.5)。此外,霉菌损坏≥0.19米的房屋与3岁时的喘息以及7岁时评估的早期短暂喘息相关(aOR=2.9;CI=1.3,6.4和aOR=3.5;CI=1.5,8.2)。霉菌损坏<0.19米和潮湿损坏<0.29米与健康结果无关。霉菌和潮湿损坏也与哮喘无关。
我们的数据表明,仅1岁时家中霉菌(≥0.19米)和潮湿损坏(≥0.29米)分析的最高类别与3岁和7岁时的喘息显著相关;然而,低于这些水平的数据过于稀疏,无法评估关系的形状或探索潜在的健康相关阈值。