Department of Pediatric Nephrology, Fundación Valle del Lili, Cali, Colombia.
Department of Pediatrics, Universidad del Cauca, Popayán, Cauca, Colombia.
PLoS One. 2020 Aug 24;15(8):e0235976. doi: 10.1371/journal.pone.0235976. eCollection 2020.
Acute kidney injury is frequent in critically ill children; however, it varies in causality and epidemiology according to the level of patient care complexity. A multicenter prospective cohort study was conducted in four medium-complexity pediatric intensive care units from the Colombian southeast aimed to estimate the clinical prognosis of patients with diagnosis of acute kidney injury.
We included children >28 days and <18 years of age, who were admitted with diagnosis of acute kidney injury classified by Kidney Disease Improving Global Outcomes (KDIGO), during the period from January to December 2017. Severe acute kidney injury was defined as stage 2 and stage 3 classifications. Maximum KDIGO was evaluated during the hospital stay and follow up. Length of hospital stay, use of mechanical ventilation and vasoactive drugs, use of renal replacement therapy, and mortality were assessed until discharge.
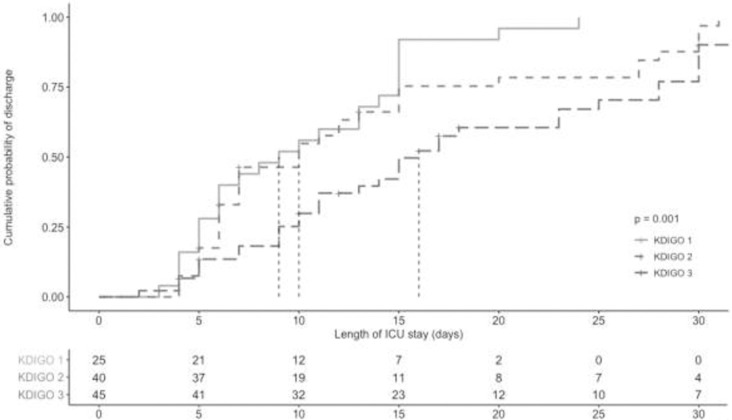
Prevalence at admission of acute kidney injury was 5.2% (95%CI 4.3% to 6.2%). It was found that 71% of the patients had their maximum KDIGO on day one; an increment in the maximum stage of acute kidney injury increased the pediatric intensive care unit stay. Patients with maximum KDIGO 3 were associated with greater use of mechanical ventilation (47%), compared with maximum KDIGO 2 (37%) and maximum KDIGO 1 (16%). Eight patients with maximum KDIGO 2 and 14 with maximum KDIGO 3 required renal replacement therapy. Mortality was at 11.8% (95%CI 6.4% to 19.4%).
Acute kidney injury, established and classified according to KDIGO as severe and its maximum stage, was associated with worse clinical outcomes; early therapeutic efforts should focus on preventing the progression to severe stages.
急性肾损伤在危重症患儿中较为常见;然而,根据患者治疗复杂程度的不同,其病因和流行病学也有所不同。本研究是在哥伦比亚东南部的四家中等复杂程度的儿科重症监护病房进行的一项多中心前瞻性队列研究,旨在评估急性肾损伤诊断患儿的临床预后。
我们纳入了 2017 年 1 月至 12 月期间因急性肾损伤(KDIGO 分类)入院的年龄>28 天且<18 岁的儿童。严重急性肾损伤定义为 2 期和 3 期分类。在住院期间和随访期间评估最大 KDIGO。评估住院时间、机械通气和血管活性药物的使用、肾脏替代治疗的使用以及死亡率,直至出院。
急性肾损伤入院时的患病率为 5.2%(95%CI 4.3%至 6.2%)。结果发现,71%的患者在第 1 天达到最大 KDIGO;急性肾损伤的最大分期增加,儿科重症监护病房的停留时间也随之增加。与最大 KDIGO 2(37%)和最大 KDIGO 1(16%)相比,最大 KDIGO 3 的患者机械通气使用率更高(47%)。14 例最大 KDIGO 3 的患者需要肾脏替代治疗。死亡率为 11.8%(95%CI 6.4%至 19.4%)。
根据 KDIGO 确定的严重程度及其最大分期的急性肾损伤与更差的临床结局相关;早期的治疗重点应放在预防疾病向严重阶段进展。