Safdar Osama Y, Shalaby Mohammed, Khathlan Norah, Elattal Bassem, Bin Joubah Mohammed, Bukahri Esraa, Saber Mafaza, Alahadal Arwa, Aljariry Hala, Gasim Safaa, Hadadi Afnan, Alqahtani Abdullah, Awleyakhan Roaa, Kari Jameela A
Pediatric Nephrology Unit, Department of Pediatrics, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia.
Pediatric Department, King Abdulaziz University Hospital, P.O. Box 14071, Alsulimania, Jeddah, 21414, Kingdom of Saudi Arabia.
BMC Nephrol. 2016 Sep 13;17(1):130. doi: 10.1186/s12882-016-0346-z.
Acute kidney injury (AKI) has been associated with high morbidity and mortality rates among critically ill children. Cystatin C is a protease inhibitor, and studies have shown that it is a promising marker for the early diagnosis of AKI. Our goal in this study was to assess whether serum cystatin C could serve as an accurate marker for the diagnosis of AKI.
This prospective study was undertaken in the pediatric intensive care unit at King Abdulaziz University Hospital. Serum creatinine and serum cystatin C levels were both measured in patients on admission (0 h) and at 6, 12, and 24 h after admission. AKI was diagnosed according to the modified pRIFLE criteria. Receiver operating characteristic (ROC) curve analysis was performed to assess the utility of serum cystatin C for diagnosing AKI.
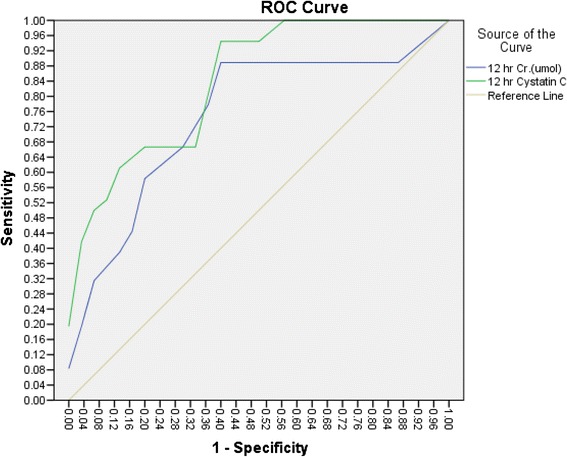
A total of 62 patients were enrolled in this study, and 32 were diagnosed with AKI according to the modified pRIFLE criteria (51.4 %). The area under the ROC curve for serum cystatin indicated that it was a good marker for the diagnosis of AKI at 0, 6, 12 and 24 h, with sensitivities of 78, 94, 94 and 83 %, respectively. However, the specificities of serum cystatin C at 0, 6, 12, and 24 h were 57, 57, 60 and 50 %, respectively. The optimal cutoff value was 0.645 mg/L. The area under the ROC for serum creatinine showed sensitivities of 50, 65.4, 69.2 and 57.7 % and specificities of 67.7, 70, 60 and 70 % at 0, 6, 12 and 24 h, respectively. The optimal cutoff value for serum creatinine was 30 μmol/l. Comparisons of ROC curves revealed that serum cystatin C was superior to serum creatinine for the diagnosis of AKI at 12 h (p = 0.03), but no differences were detected at 0, 6 or 24 h.
Serum cystatin is a sensitive, but not a specific, marker for the diagnosis of AKI in critically ill children.
急性肾损伤(AKI)与危重症儿童的高发病率和死亡率相关。胱抑素C是一种蛋白酶抑制剂,研究表明它是早期诊断AKI的一个有前景的标志物。本研究的目的是评估血清胱抑素C是否可作为诊断AKI的准确标志物。
本前瞻性研究在阿卜杜勒阿齐兹国王大学医院儿科重症监护病房进行。在患者入院时(0小时)以及入院后6、12和24小时测量血清肌酐和血清胱抑素C水平。根据改良的pRIFLE标准诊断AKI。进行受试者操作特征(ROC)曲线分析以评估血清胱抑素C对诊断AKI的效用。
本研究共纳入62例患者,根据改良的pRIFLE标准,32例被诊断为AKI(51.4%)。血清胱抑素的ROC曲线下面积表明,它在0、6、12和24小时是诊断AKI的良好标志物,敏感性分别为78%、94%、94%和83%。然而,血清胱抑素C在0、6、12和24小时的特异性分别为57%、57%、60%和50%。最佳截断值为0.645mg/L。血清肌酐的ROC曲线下面积在0、6、12和24小时的敏感性分别为50%、65.4%、69.2%和57.7%,特异性分别为67.7%、70%、60%和70%。血清肌酐的最佳截断值为30μmol/l。ROC曲线比较显示,血清胱抑素C在12小时诊断AKI方面优于血清肌酐(p = 0.03),但在0、6或24小时未检测到差异。
血清胱抑素是危重症儿童诊断AKI的一个敏感但非特异性的标志物。