Omere Chasey, Richardson Lauren, Saade George R, Bonney Elizabeth A, Kechichian Talar, Menon Ramkumar
Division of Maternal-Fetal Medicine and Perinatal Research, Department of Obstetrics & Gynecology, The University of Texas Medical Branch at Galveston, Galveston, TX, United States.
Department of Obstetrics, Gynecology and Reproductive Sciences, College of Medicine, The University of Vermont, Burlington, VT, United States.
Front Physiol. 2020 Jul 24;11:891. doi: 10.3389/fphys.2020.00891. eCollection 2020.
Protection of the fetus within the amniotic sac is primarily attained by remodeling fetal membrane (amniochorion) cells through cyclic epithelial to mesenchymal and mesenchymal to epithelial (EMT and MET) transitions. Endocrine and paracrine factors regulate EMT and MET during pregnancy. At term, increased oxidative stress forces a terminal state of EMT and inflammation, predisposing to membrane weakening and rupture. IL-6 is a constitutively expressed cytokine during gestation, but it is elevated in term and preterm births. Therefore, we tested the hypothesis that IL-6 can determine the fate of amnion membrane cells and that pathologic levels of IL-6 can cause a terminal state of EMT and inflammation, leading to adverse pregnancy outcomes.
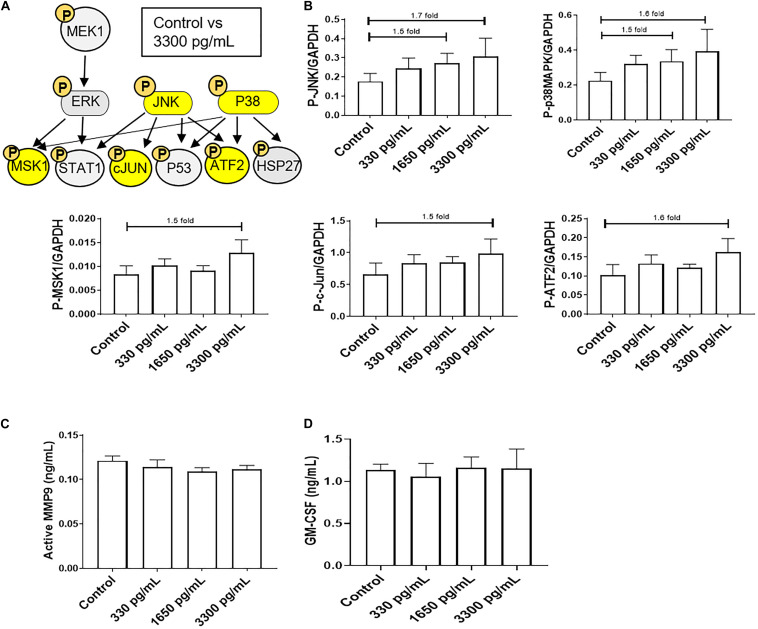
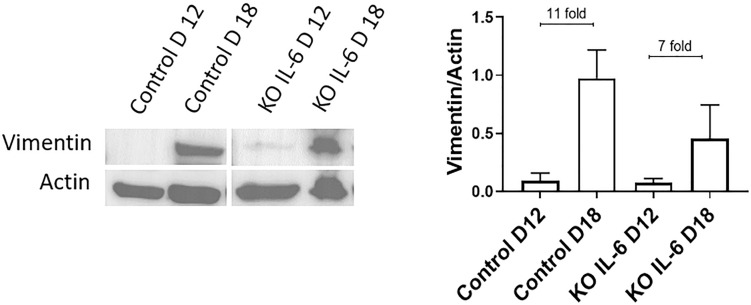
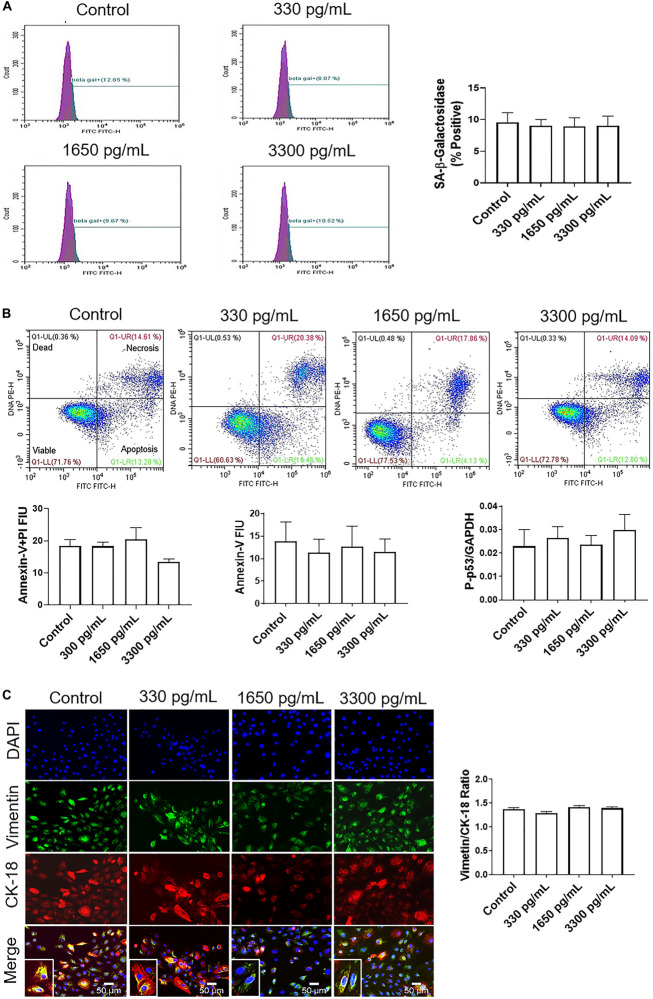
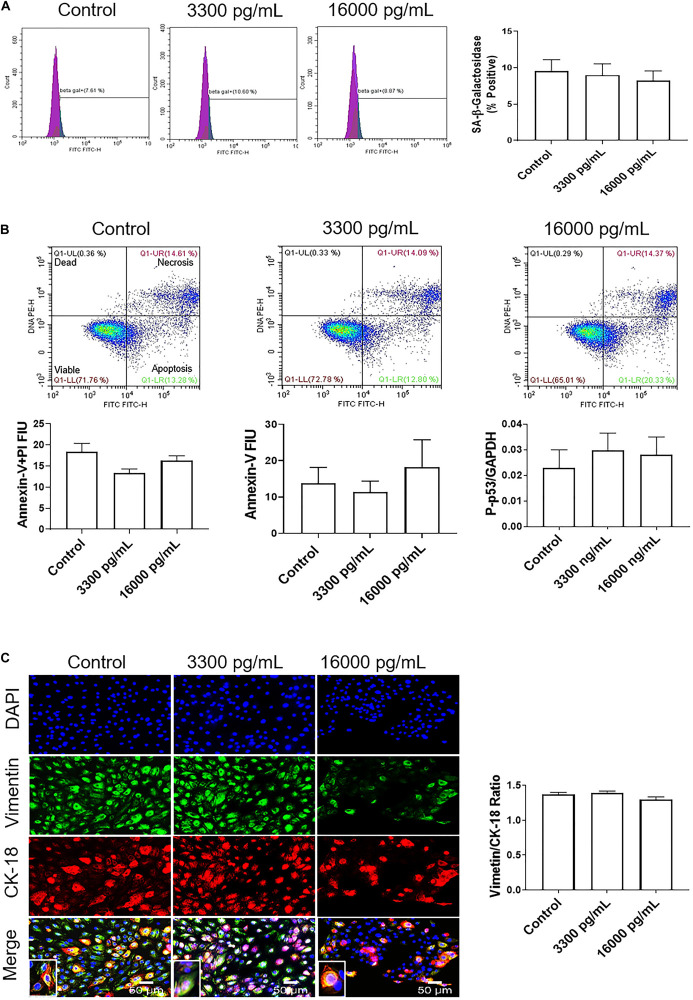
Primary amnion epithelial cells (AECs) were treated with recombinant IL-6 (330, 1,650, 3,330, and 16,000 pg/ml) for 48 h ( = 5). IL-6-induced cell senescence (aging), cell death (apoptosis and necrosis), and cell cycle changes were studied using flow cytometry. Cellular transitions were determined by immunocytochemistry and western blot analysis, while IL-6 signaling (activation of signaling kinases) was measured by immunoassay. Inflammatory marker matrix metalloproteinase (MMP9) and granulocyte-macrophage colony-stimulating factor (GM-CSF) concentrations were measured using a Fluorokine E assay and ELISA, respectively. Amniotic membranes collected on gestational day (D) 12 and D18 from IL-6 knockout (KO) and control C57BL/6 mice ( = 3 each) were used to determine the impact of IL-6 on cell transitions. Fold changes were measured based on the mean of each group.
IL-6 treatment of AECs at physiologic or pathologic doses increased JNK and p38MAPK activation; however, the activation of signals did not cause changes in AEC cell cycle, cellular senescence, apoptosis, necrosis, cellular transitions, or inflammation (MMP9 and GM-CSF) compared to control. EMT markers were higher on D18 compared to D12 regardless of IL-6 status in the mouse amniotic sac.
Physiologic and pathologic concentrations of IL-6 did not cause amnion cell aging, cell death, cellular transitions, or inflammation. IL-6 may function to maintain cellular homeostasis throughout gestation in fetal membrane cells. Although IL-6 is a good biomarker for adverse pregnancies, it is not an indicator of an underlying pathological mechanism in membrane cells.
羊膜囊内胎儿的保护主要通过胎儿膜(羊膜绒毛膜)细胞通过周期性上皮-间充质和间充质-上皮(EMT和MET)转变进行重塑来实现。内分泌和旁分泌因子在孕期调节EMT和MET。足月时,氧化应激增加迫使EMT和炎症进入终末状态,易导致胎膜弱化和破裂。白细胞介素-6(IL-6)是孕期持续表达的细胞因子,但在足月和早产时其水平会升高。因此,我们检验了以下假设:IL-6可决定羊膜细胞的命运,且IL-6的病理水平可导致EMT和炎症的终末状态,从而导致不良妊娠结局。
将原代羊膜上皮细胞(AECs)用重组IL-6(330、1650、3330和16000 pg/ml)处理48小时(n = 5)。使用流式细胞术研究IL-6诱导的细胞衰老(老化)、细胞死亡(凋亡和坏死)及细胞周期变化。通过免疫细胞化学和蛋白质印迹分析确定细胞转变,同时通过免疫测定法检测IL-6信号传导(信号激酶的激活)。分别使用荧光素酶E测定法和酶联免疫吸附测定法(ELISA)测量炎症标志物基质金属蛋白酶(MMP9)和粒细胞-巨噬细胞集落刺激因子(GM-CSF)的浓度。使用从IL-6基因敲除(KO)和对照C57BL/6小鼠(每组n = 3)在妊娠第12天和第18天收集的羊膜来确定IL-6对细胞转变 的影响。基于每组的平均值测量倍数变化。
以生理或病理剂量用IL-6处理AECs会增加JNK和p38MAPK的激活;然而,与对照相比,信号激活并未引起AEC细胞周期、细胞衰老、凋亡、坏死、细胞转变或炎症(MMP9和GM-CSF)的变化。无论小鼠羊膜囊中IL-6状态如何,与妊娠第12天相比,妊娠第18天的EMT标志物更高。
生理和病理浓度的IL-6均未引起羊膜细胞衰老、细胞死亡、细胞转变或炎症。IL-6可能在整个孕期维持胎膜细胞的细胞稳态。尽管IL-6是不良妊娠的良好生物标志物,但它不是胎膜细胞潜在病理机制的指标。