Department of Medicine, Duke University School of Medicine, Durham, North Carolina.
Center for the Study of Aging and Human Development, Duke University Medical Center, Durham, North Carolina.
J Am Geriatr Soc. 2020 Nov;68(11):2650-2655. doi: 10.1111/jgs.16800. Epub 2020 Aug 27.
To develop a prognostic model for hospital admissions over a 1-year period among community-dwelling older adults with self-reported hearing and/or vision impairments based on readily obtainable clinical predictors.
Retrospective cohort study.
Medicare Current Beneficiary Survey from 1999 to 2006.
Community-dwelling Medicare beneficiaries, aged 65 years and older, with self-reported hearing and/or vision impairment (N = 15,999).
The primary outcome was any hospital admission over a predefined 1-year study period. Candidate predictors included demographic factors, prior healthcare utilization, comorbidities, functional impairment, and patient-level factors. We analyzed the association of all candidate predictors with any hospital admission over the 1-year study period using multivariable logistic regression. The final model was created using a penalized regression method known as the least absolute shrinkage and selection operator. Model performance was assessed by discrimination (concordance statistic (c-statistic)) and calibration (evaluated graphically). Internal validation was performed via bootstrapping, and results were adjusted for overoptimism.
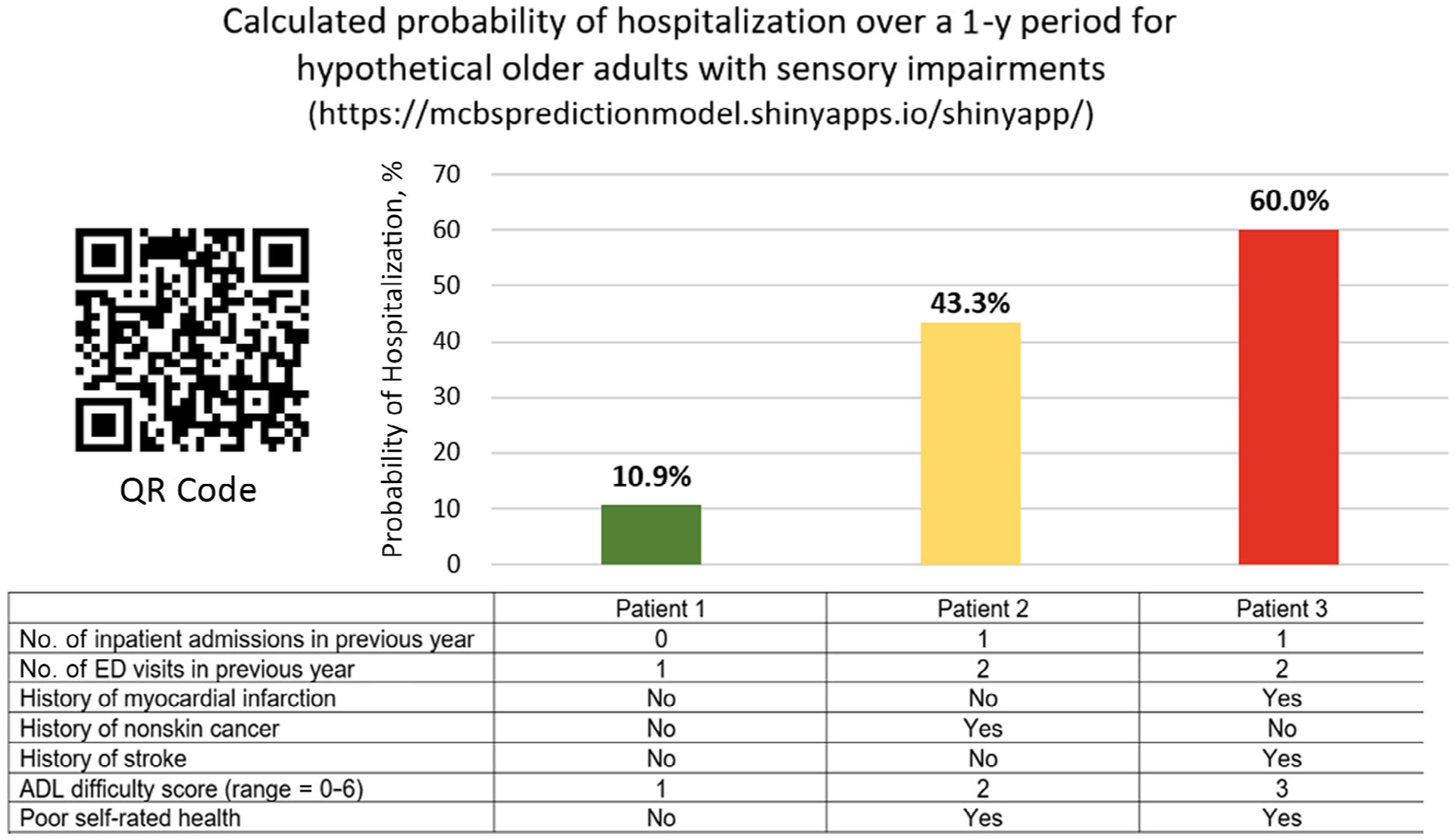
Of the 15,999 participants, the mean age was 78 years and 55% were female. A total of 2,567 participants (16.0%) had at least one hospital admission in the 1-year study period. The final model included seven variables independently associated with hospitalization: number of inpatient admissions in the previous year, number of emergency department visits in the previous year, activities of daily living difficulty score, poor self-rated health, and self-reported history of myocardial infarction, stroke, and nonskin cancer. The c-statistic of the final model was 0.717. The optimism-corrected c-statistic after bootstrap internal validation was 0.716. A calibration plot suggested that the model tended to overestimate risk among patients at the highest risk for hospitalization.
This prognostic model can help identify which community-dwelling older adults with sensory impairments are at highest risk for hospitalization and may inform allocation of healthcare resources.
基于易于获得的临床预测因素,为有自我报告听力和/或视力障碍的社区居住的老年患者建立 1 年内住院的预后模型。
回顾性队列研究。
1999 年至 2006 年的医疗保险当前受益人调查。
年龄在 65 岁及以上、有自我报告听力和/或视力障碍的社区居住的医疗保险受益人(N=15999)。
主要结局是在预先确定的 1 年研究期间内任何医院就诊。候选预测因素包括人口统计学因素、先前的医疗保健利用情况、合并症、功能障碍和患者层面的因素。我们使用多变量逻辑回归分析所有候选预测因素与 1 年内任何医院就诊的关联。使用称为最小绝对收缩和选择算子(least absolute shrinkage and selection operator)的惩罚回归方法创建最终模型。通过区分(一致性统计量(concordance statistic)(c 统计量))和校准(图形评估)评估模型性能。通过引导法进行内部验证,并调整结果以消除过拟合。
在 15999 名参与者中,平均年龄为 78 岁,55%为女性。共有 2567 名(16.0%)参与者在 1 年研究期间至少有 1 次住院。最终模型纳入了 7 个与住院相关的独立变量:前一年的住院次数、前一年的急诊就诊次数、日常生活活动能力评分、自我报告的健康状况较差,以及自我报告的心肌梗死、中风和非皮肤癌病史。最终模型的 c 统计量为 0.717。引导法内部验证后的校正 c 统计量为 0.716。校准图表明,该模型倾向于高估住院风险最高的患者的风险。
该预后模型可帮助识别有感官障碍的社区居住的老年患者中哪些患者住院风险最高,并为医疗资源分配提供信息。