Department of Medicine, Duke University School of Medicine, Durham, North Carolina.
Center for the Study of Aging and Human Development, Duke University Medical Center, Durham, North Carolina.
J Am Geriatr Soc. 2019 Aug;67(8):1617-1624. doi: 10.1111/jgs.15891. Epub 2019 Mar 29.
To examine the association between self-reported vision impairment (VI), hearing impairment (HI), and dual-sensory impairment (DSI), stratified by dementia status, on hospital admissions, hospice use, and healthcare costs.
Retrospective analysis.
Medicare Current Beneficiary Survey from 1999 to 2006.
Rotating panel of community-dwelling Medicare beneficiaries, aged 65 years and older (N = 24 009).
VI and HI were ascertained by self-report. Dementia status was determined by self-report or diagnosis codes in claims data. Primary outcomes included any inpatient admission over a 2-year period, hospice use over a 2-year period, annual Medicare fee-for-service costs, and total healthcare costs (which included information from Medicare claims data and other self-reported payments).
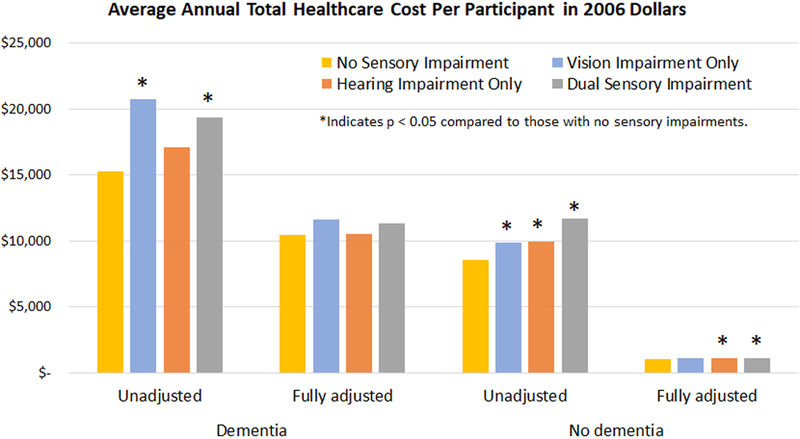
Self-reported DSI was present in 30.2% (n = 263/871) of participants with dementia and 17.8% (n = 4112/23 138) of participants without dementia. In multivariable logistic regression models, HI, VI, or DSI was generally associated with increased odds of hospitalization and hospice use regardless of dementia status. In a generalized linear model adjusted for demographics, annual total healthcare costs were greater for those with DSI and dementia compared to those with DSI without dementia ($28 875 vs $3340, respectively). Presence of any sensory impairment was generally associated with higher healthcare costs. In a model adjusted for demographics, Medicaid status, and chronic medical conditions, DSI compared with no sensory impairment was associated with a small, but statistically significant, difference in total healthcare spending in those without dementia ($1151 vs $1056; P < .001) but not in those with dementia ($11 303 vs $10 466; P = .395).
Older adults with sensory and cognitive impairments constitute a particularly prevalent and vulnerable population who are at increased risk of hospitalization and contribute to higher healthcare spending. J Am Geriatr Soc 67:1617-1624, 2019.
根据痴呆症的状态,研究自我报告的视力障碍(VI)、听力障碍(HI)和双重感觉障碍(DSI)与住院、临终关怀使用和医疗保健费用之间的关联。
回顾性分析。
1999 年至 2006 年的医疗保险当前受益人调查。
年龄在 65 岁及以上的居住在社区的医疗保险受益人(N=24009)。
VI 和 HI 通过自我报告确定。痴呆症状态通过自我报告或索赔数据中的诊断代码确定。主要结果包括在 2 年内任何一次住院、在 2 年内使用临终关怀、每年的医疗保险按服务收费成本以及总医疗保健费用(包括医疗保险索赔数据和其他自我报告支付的信息)。
自我报告的 DSI 存在于 30.2%(n=263/871)患有痴呆症的参与者和 17.8%(n=4112/23138)没有痴呆症的参与者中。在多变量逻辑回归模型中,HI、VI 或 DSI 通常与住院和临终关怀使用的几率增加相关,无论痴呆症状态如何。在调整人口统计学因素的广义线性模型中,与没有 DSI 但患有痴呆症的人相比,患有 DSI 和痴呆症的人每年的总医疗保健费用更高(分别为 28875 美元和 3340 美元)。任何感觉障碍的存在通常与更高的医疗保健费用相关。在调整人口统计学因素、医疗补助状况和慢性疾病的模型中,与没有感觉障碍相比,患有 DSI 的人在没有痴呆症的人中与总医疗保健支出的差异较小,但具有统计学意义(1151 美元对 1056 美元;P<0.001),但在患有痴呆症的人中没有差异(11303 美元对 10466 美元;P=0.395)。
有感觉和认知障碍的老年人是一个特别普遍和脆弱的群体,他们的住院风险增加,并导致更高的医疗保健支出。美国老年学会杂志 67:1617-1624,2019。