Department of Paediatrics, Leiden University Medical Center, Leiden, The Netherlands.
Department of Pathology, Radboud University Medical Center, Nijmegen, The Netherlands.
J Pathol Clin Res. 2021 Jan;7(1):10-26. doi: 10.1002/cjp2.177. Epub 2020 Aug 27.
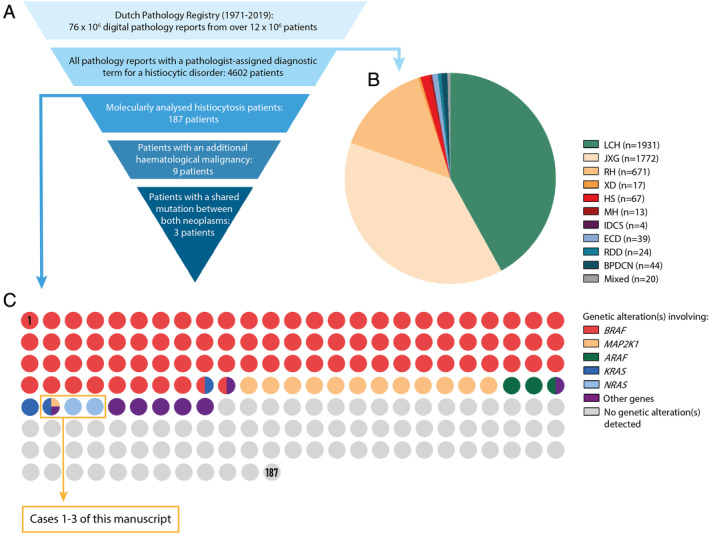
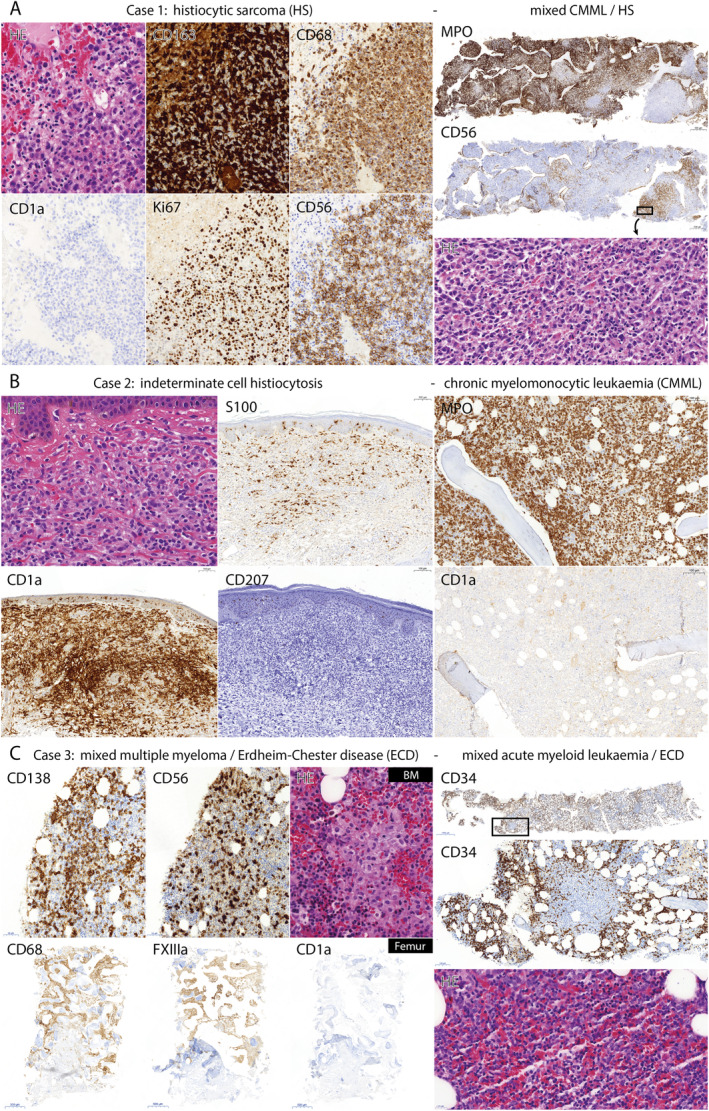
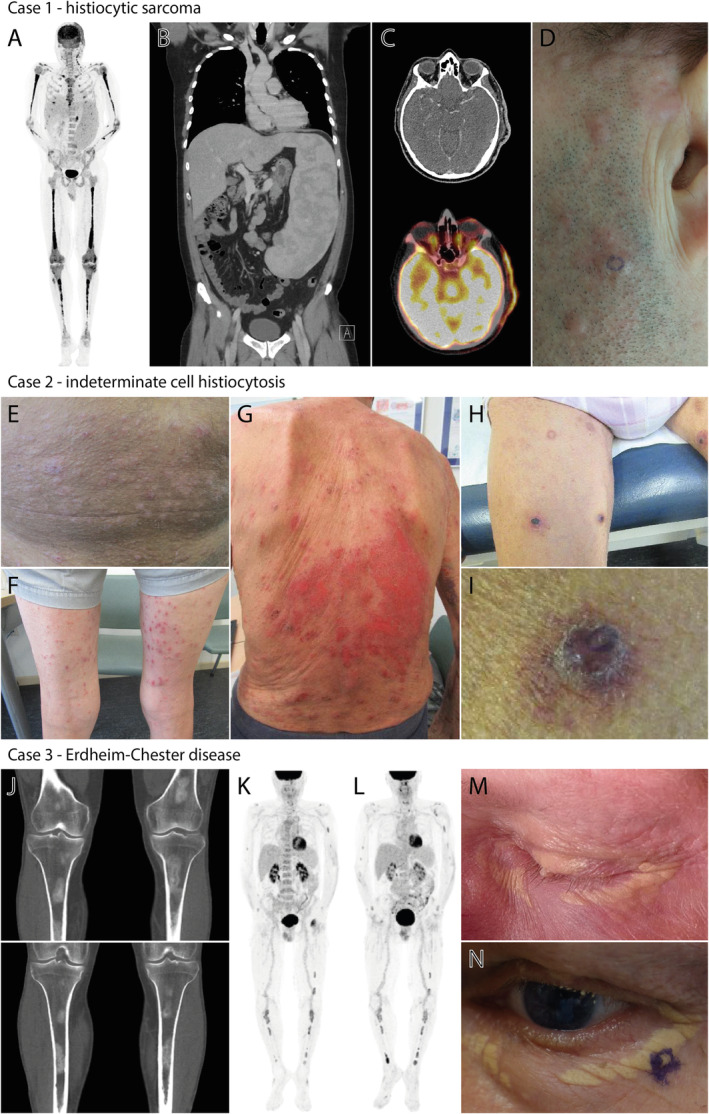
Histiocytic disorders are a spectrum of rare diseases characterised by the accumulation of macrophage-, dendritic cell-, or monocyte-differentiated cells in various tissues and organs. The discovery of recurrent genetic alterations in many of these histiocytoses has led to their recognition as clonal neoplastic diseases. Moreover, the identification of the same somatic mutation in histiocytic lesions and peripheral blood and/or bone marrow cells from histiocytosis patients has provided evidence for systemic histiocytic neoplasms to originate from haematopoietic stem/progenitor cells (HSPCs). Here, we investigated associations between histiocytic disorders and additional haematological malignancies bearing the same genetic alteration(s) using the nationwide Dutch Pathology Registry. By searching on pathologist-assigned diagnostic terms for the various histiocytic disorders, we identified 4602 patients with a putative histopathological diagnosis of a histiocytic disorder between 1971 and 2019. Histiocytosis-affected tissue samples of 187 patients had been analysed for genetic alterations as part of routine molecular diagnostics, including from nine patients with an additional haematological malignancy. Among these patients, we discovered three cases with different histiocytic neoplasms and additional haematological malignancies bearing identical oncogenic mutations, including one patient with concomitant KRAS p.A59E mutated histiocytic sarcoma and chronic myelomonocytic leukaemia (CMML), one patient with synchronous NRAS p.G12V mutated indeterminate cell histiocytosis and CMML, and one patient with subsequent NRAS p.Q61R mutated Erdheim-Chester disease and acute myeloid leukaemia. These cases support the existence of a common haematopoietic cell-of-origin in at least a proportion of patients with a histiocytic neoplasm and additional haematological malignancy. In addition, they suggest that driver mutations in particular genes (e.g. N/KRAS) may specifically predispose to the development of an additional clonally related haematological malignancy or secondary histiocytic neoplasm. Finally, the putative existence of derailed multipotent HSPCs in these patients emphasises the importance of adequate (bone marrow) staging, molecular analysis and long-term follow-up of all histiocytosis patients.
组织细胞疾病是一组罕见疾病,其特征是巨噬细胞、树突状细胞或单核细胞分化细胞在各种组织和器官中积累。许多组织细胞疾病中反复出现的遗传改变的发现,导致它们被认为是克隆性肿瘤性疾病。此外,在组织细胞病变和组织细胞病患者的外周血和/或骨髓细胞中发现相同的体细胞突变,为系统性组织细胞肿瘤起源于造血干/祖细胞(HSPCs)提供了证据。在这里,我们使用全国性的荷兰病理学登记处,研究了具有相同遗传改变的其他血液系统恶性肿瘤与组织细胞疾病之间的关联。通过搜索病理学家分配的各种组织细胞疾病的诊断术语,我们在 1971 年至 2019 年间确定了 4602 名疑似组织病理学诊断为组织细胞疾病的患者。187 名组织细胞疾病患者的受影响组织样本已进行了遗传改变分析,作为常规分子诊断的一部分,其中包括 9 名患有其他血液系统恶性肿瘤的患者。在这些患者中,我们发现了三例具有不同组织细胞肿瘤和具有相同致癌突变的其他血液系统恶性肿瘤的病例,包括一名同时患有 KRAS p.A59E 突变的组织细胞肉瘤和慢性髓单核细胞白血病(CMML)、一名患有同步 NRAS p.G12V 突变的不定细胞组织细胞增生症和 CMML 的患者,以及一名患有随后的 NRAS p.Q61R 突变的 Erdheim-Chester 病和急性髓系白血病的患者。这些病例支持至少一部分组织细胞肿瘤和其他血液系统恶性肿瘤患者存在共同的造血细胞起源。此外,它们表明特定基因(例如 N/KRAS)中的驱动突变可能特别容易导致额外的克隆相关血液系统恶性肿瘤或继发性组织细胞肿瘤的发展。最后,这些患者中存在失调的多能性 HSPCs,强调了对所有组织细胞病患者进行充分(骨髓)分期、分子分析和长期随访的重要性。