Department of Molecular Neurology, University Hospital Erlangen, Schwabachanlage 6, 91054, Erlangen, Germany.
Center for Rare Diseases Erlangen (ZSEER), University Hospital Erlangen, Erlangen, Germany.
BMC Neurol. 2020 Aug 29;20(1):321. doi: 10.1186/s12883-020-01891-1.
Anterior spinal cord herniation (aSCH) is a rare cause of myelopathy which may present as pure motor syndrome and mimic other degenerative diseases of the spinal cord. In slowly progressive cases, diagnosis may be impeded by equivocal imaging results and mistaken for evolving upper motor neuron disease. As early imaging studies are lacking, we aimed to provide a detailed description of imaging and neurophysiology findings in a patient with aSCH, focusing on the early symptomatic stages.
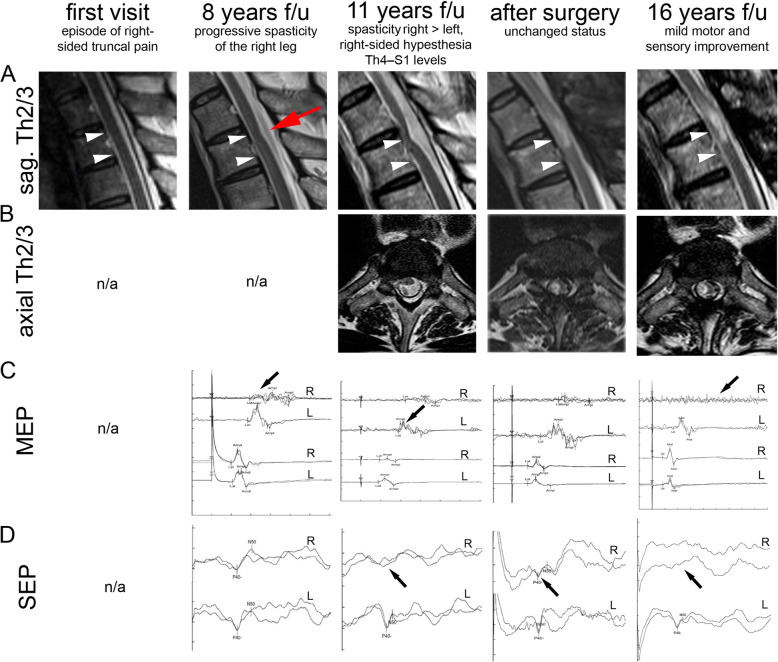
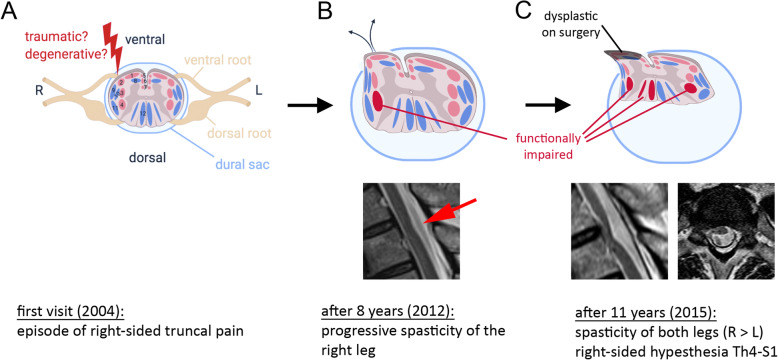
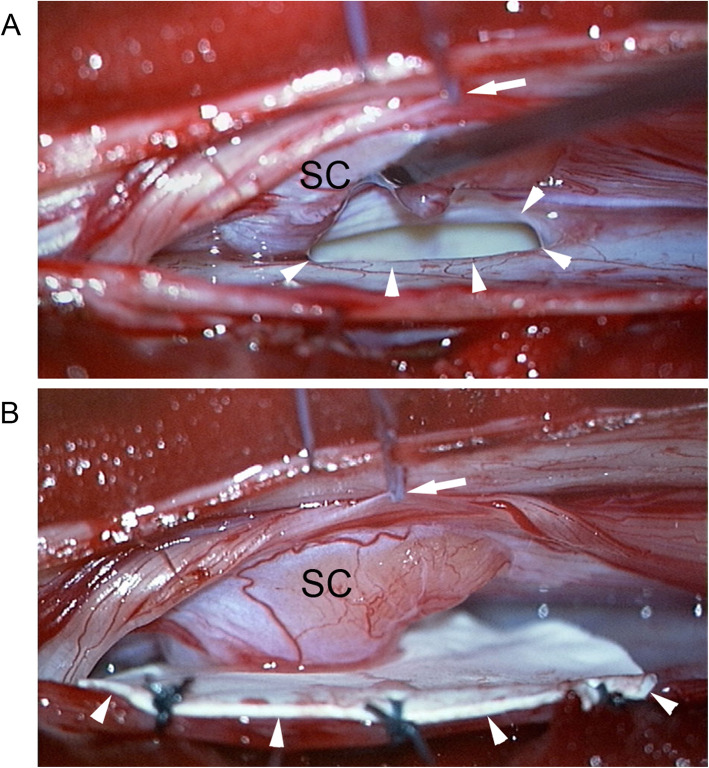
We here present the case of a 51-year old male patient with an episode of pain in the right trunk and a normal spinal MRI. After a symptom-free interval of 8 years, spasticity and paresis evolved in the right leg. There was subtle ventral displacement and posterior indentation of the thoracic spinal cord on MRI which, in retrospect, was missed as an early sign of aSCH. After another 3 years, symptoms spread to the left leg and a sensory deficit of the trunk became evident. Follow-up MRI now clearly showed an aSCH. Neurosurgical intervention consisted of remobilization of the herniated spinal cord and patch closure of the dura defect. Over the following years, motor and sensory symptoms partially improved.
The history of this patient with aSCH illustrates the importance of careful longitudinal clinical follow-up with repeated imaging studies in progressive upper motor neuron syndromes. Specific attention should be paid to a history of truncal pain and to MRI findings of a ventrally displaced spinal cord. Neurosurgical intervention may halt the progression of herniation.
脊髓前中央管突出症(aSCH)是一种罕见的引起脊髓病的原因,可能表现为单纯运动综合征,并与脊髓的其他退行性疾病相混淆。在进展缓慢的病例中,由于影像学结果不明确,可能会妨碍诊断,并误诊为进展性上运动神经元疾病。由于早期影像学研究的缺乏,我们旨在详细描述 aSCH 患者的影像学和神经生理学表现,重点关注早期症状阶段。
我们在此介绍一名 51 岁男性患者的病例,他曾出现右侧躯干疼痛,且脊髓 MRI 正常。8 年后无症状期,右腿出现痉挛和无力。MRI 显示胸段脊髓轻微腹侧移位和后向凹陷,但这被视为 aSCH 的早期征象而被遗漏。又过了 3 年后,症状扩散到左腿,躯干感觉缺陷变得明显。随访 MRI 现在清楚地显示了 aSCH。神经外科干预包括重新移动突出的脊髓和修补硬脑膜缺损。在随后的几年中,运动和感觉症状部分改善。
该 aSCH 患者的病史说明了在进行性上运动神经元综合征中,仔细的纵向临床随访和重复影像学研究的重要性。应特别注意躯干疼痛的病史和 MRI 发现的脊髓腹侧移位。神经外科干预可能会阻止突出的进展。