Lancet. 2020 Oct 17;396(10258):1250-1284. doi: 10.1016/S0140-6736(20)30750-9. Epub 2020 Aug 27.
Achieving universal health coverage (UHC) involves all people receiving the health services they need, of high quality, without experiencing financial hardship. Making progress towards UHC is a policy priority for both countries and global institutions, as highlighted by the agenda of the UN Sustainable Development Goals (SDGs) and WHO's Thirteenth General Programme of Work (GPW13). Measuring effective coverage at the health-system level is important for understanding whether health services are aligned with countries' health profiles and are of sufficient quality to produce health gains for populations of all ages.
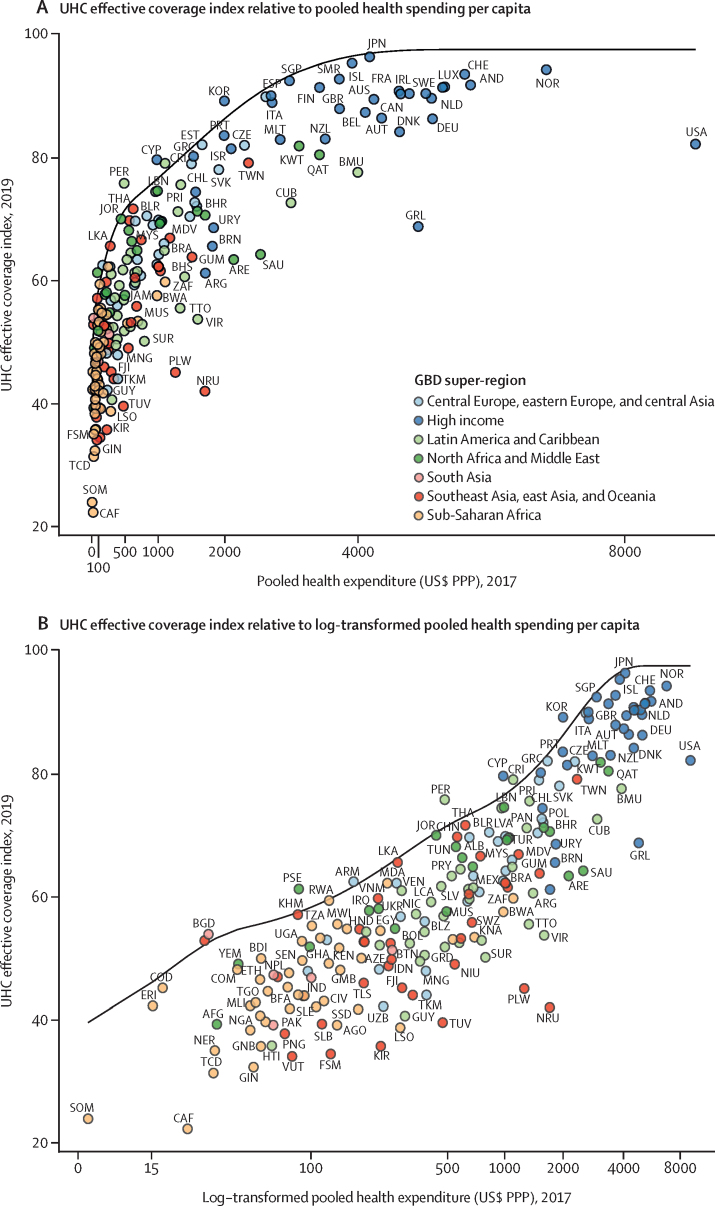
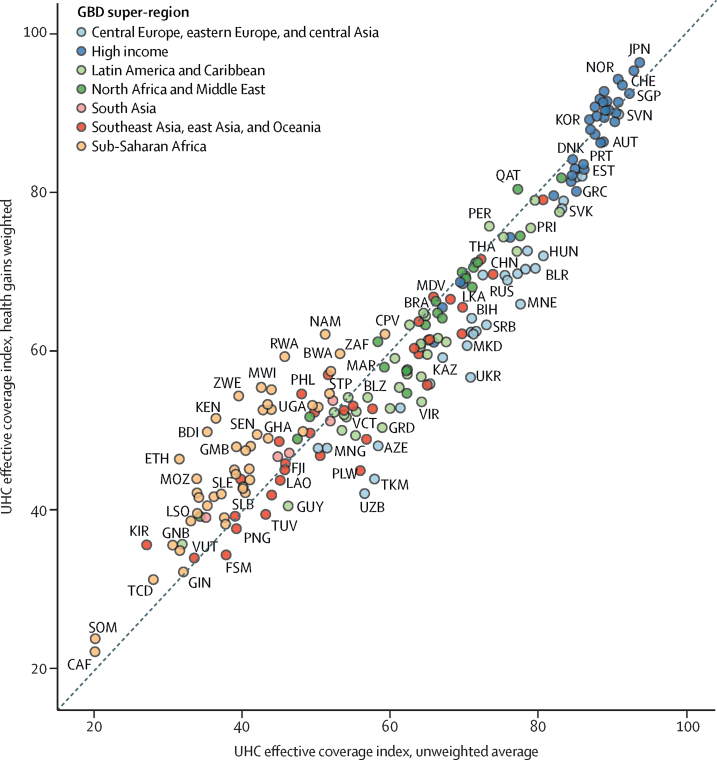
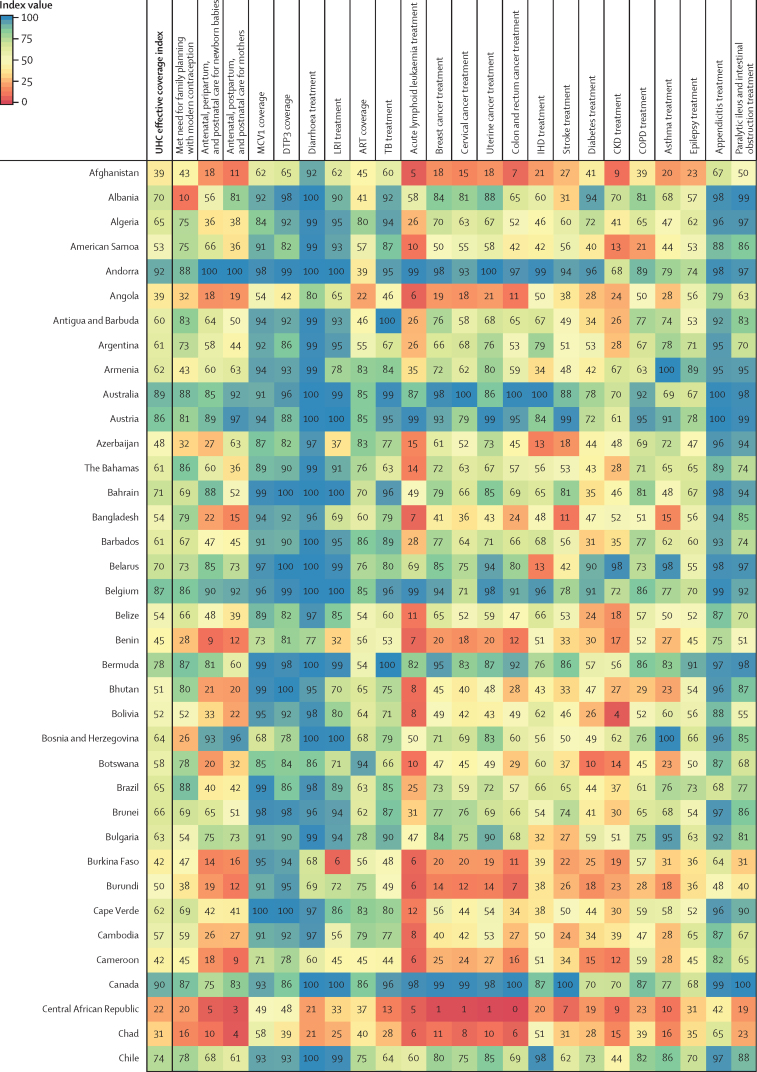
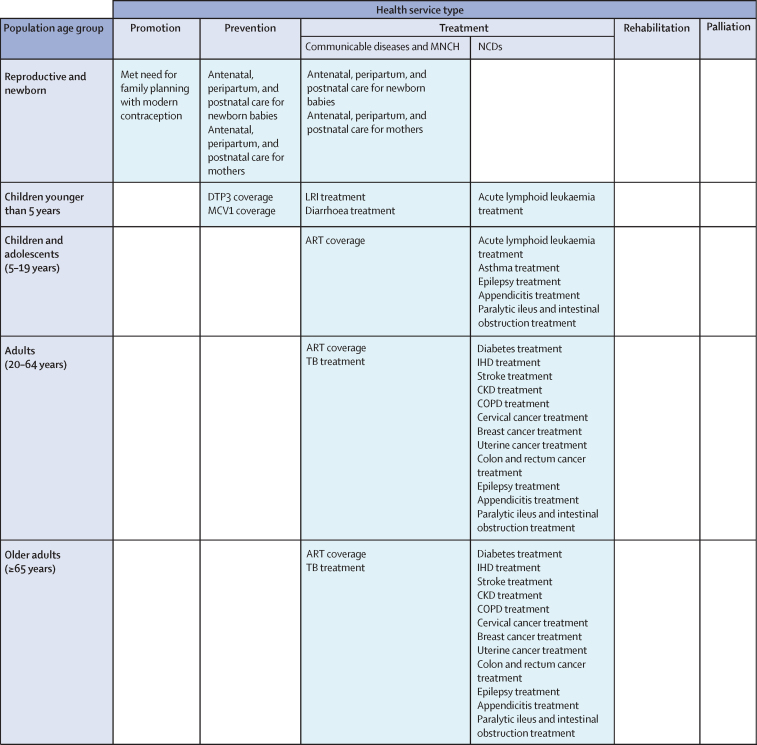
Based on the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, we assessed UHC effective coverage for 204 countries and territories from 1990 to 2019. Drawing from a measurement framework developed through WHO's GPW13 consultation, we mapped 23 effective coverage indicators to a matrix representing health service types (eg, promotion, prevention, and treatment) and five population-age groups spanning from reproductive and newborn to older adults (≥65 years). Effective coverage indicators were based on intervention coverage or outcome-based measures such as mortality-to-incidence ratios to approximate access to quality care; outcome-based measures were transformed to values on a scale of 0-100 based on the 2·5th and 97·5th percentile of location-year values. We constructed the UHC effective coverage index by weighting each effective coverage indicator relative to its associated potential health gains, as measured by disability-adjusted life-years for each location-year and population-age group. For three tests of validity (content, known-groups, and convergent), UHC effective coverage index performance was generally better than that of other UHC service coverage indices from WHO (ie, the current metric for SDG indicator 3.8.1 on UHC service coverage), the World Bank, and GBD 2017. We quantified frontiers of UHC effective coverage performance on the basis of pooled health spending per capita, representing UHC effective coverage index levels achieved in 2019 relative to country-level government health spending, prepaid private expenditures, and development assistance for health. To assess current trajectories towards the GPW13 UHC billion target-1 billion more people benefiting from UHC by 2023-we estimated additional population equivalents with UHC effective coverage from 2018 to 2023.
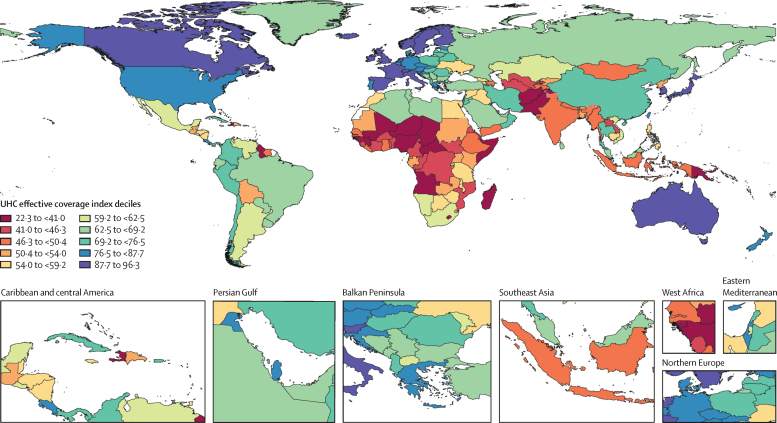
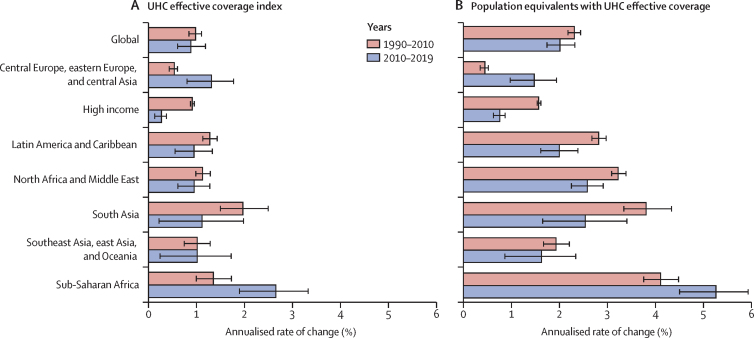
Globally, performance on the UHC effective coverage index improved from 45·8 (95% uncertainty interval 44·2-47·5) in 1990 to 60·3 (58·7-61·9) in 2019, yet country-level UHC effective coverage in 2019 still spanned from 95 or higher in Japan and Iceland to lower than 25 in Somalia and the Central African Republic. Since 2010, sub-Saharan Africa showed accelerated gains on the UHC effective coverage index (at an average increase of 2·6% [1·9-3·3] per year up to 2019); by contrast, most other GBD super-regions had slowed rates of progress in 2010-2019 relative to 1990-2010. Many countries showed lagging performance on effective coverage indicators for non-communicable diseases relative to those for communicable diseases and maternal and child health, despite non-communicable diseases accounting for a greater proportion of potential health gains in 2019, suggesting that many health systems are not keeping pace with the rising non-communicable disease burden and associated population health needs. In 2019, the UHC effective coverage index was associated with pooled health spending per capita (r=0·79), although countries across the development spectrum had much lower UHC effective coverage than is potentially achievable relative to their health spending. Under maximum efficiency of translating health spending into UHC effective coverage performance, countries would need to reach $1398 pooled health spending per capita (US$ adjusted for purchasing power parity) in order to achieve 80 on the UHC effective coverage index. From 2018 to 2023, an estimated 388·9 million (358·6-421·3) more population equivalents would have UHC effective coverage, falling well short of the GPW13 target of 1 billion more people benefiting from UHC during this time. Current projections point to an estimated 3·1 billion (3·0-3·2) population equivalents still lacking UHC effective coverage in 2023, with nearly a third (968·1 million [903·5-1040·3]) residing in south Asia.
The present study demonstrates the utility of measuring effective coverage and its role in supporting improved health outcomes for all people-the ultimate goal of UHC and its achievement. Global ambitions to accelerate progress on UHC service coverage are increasingly unlikely unless concerted action on non-communicable diseases occurs and countries can better translate health spending into improved performance. Focusing on effective coverage and accounting for the world's evolving health needs lays the groundwork for better understanding how close-or how far-all populations are in benefiting from UHC.
Bill & Melinda Gates Foundation.
实现全民健康覆盖(UHC)涉及所有人都能获得高质量的卫生服务,而不会面临经济困难。推进 UHC 是国家和全球机构的政策优先事项,这一点在联合国可持续发展目标(SDG)和世卫组织第十三届总规划(GPW13)议程中得到了强调。衡量卫生系统层面的有效覆盖情况对于了解卫生服务是否与各国的卫生状况相符,以及是否足以改善各年龄段人群的健康状况非常重要。
我们根据 2019 年全球疾病、伤害和风险因素研究(GBD),评估了 204 个国家和地区从 1990 年到 2019 年的 UHC 有效覆盖情况。根据世卫组织 GPW13 咨询会议制定的测量框架,我们将 23 个有效覆盖指标映射到一个代表卫生服务类型(如促进、预防和治疗)和五个涵盖从生殖和新生儿到老年人(≥65 岁)的人口年龄组的矩阵上。有效覆盖指标基于干预覆盖或基于结果的措施,例如死亡率与发病率的比值,以近似获得高质量的护理;基于结果的措施被转换为基于位置-年份值的 2.5%和 97.5%分位数的 0-100 之间的值。我们通过将每个有效覆盖指标相对于与其相关的潜在健康收益进行加权,构建了 UHC 有效覆盖指数,这些潜在健康收益是根据每个位置-年份和人口年龄组的残疾调整生命年来衡量的。对于三项有效性测试(内容、已知群体和收敛性),UHC 有效覆盖指数的表现总体上优于世卫组织(即,SDG 指标 3.8.1 关于 UHC 服务覆盖的当前指标)、世界银行和 GBD 2017 的其他 UHC 服务覆盖指数。我们根据人均卫生支出的前沿水平,量化了 2019 年 UHC 有效覆盖指数水平相对于国家一级政府卫生支出、预付款私人支出和卫生发展援助所实现的 UHC 有效覆盖的情况,代表了 2019 年 UHC 有效覆盖的情况。为了评估到 2023 年实现 GPW13 UHC 十亿目标——使 10 亿人受益于 UHC 的当前轨迹,我们估计了 2018 年至 2023 年期间 UHC 有效覆盖的额外人口当量。
全球范围内,UHC 有效覆盖指数从 1990 年的 45.8(95%不确定性区间 44.2-47.5)提高到 2019 年的 60.3(58.7-61.9),但 2019 年各国的 UHC 有效覆盖范围仍从日本和冰岛的 95 或更高,到索马里和中非共和国的低于 25。自 2010 年以来,撒哈拉以南非洲地区在 UHC 有效覆盖指数方面的增长速度加快(平均每年增长 2.6%[1.9-3.3],直至 2019 年);相比之下,2010-2019 年期间,大多数其他 GBD 超级区域的进展速度都有所放缓。尽管非传染性疾病在 2019 年占潜在健康收益的比例更大,表明许多卫生系统没有跟上非传染性疾病负担不断增加和相关人口健康需求的步伐,但许多国家在非传染性疾病有效覆盖指标方面的表现滞后于传染性疾病和母婴健康方面的表现。2019 年,UHC 有效覆盖指数与人均卫生支出(r=0.79)相关,尽管各国在卫生支出方面的发展情况各不相同,但与实现 UHC 的潜在支出相比,它们的 UHC 有效覆盖水平要低得多。在最大效率地将卫生支出转化为 UHC 有效覆盖绩效的情况下,各国需要达到人均 1398 美元的卫生支出(经购买力平价调整后的美元),才能使 UHC 有效覆盖指数达到 80。从 2018 年到 2023 年,估计将有 3.889 亿(3.586-4.213)更多的人口当量具有 UHC 有效覆盖,远低于 GPW13 在这段时间内使 10 亿人受益于 UHC 的目标。目前的预测表明,到 2023 年,仍将有估计的 31 亿(3.0-3.2)人口当量缺乏 UHC 有效覆盖,其中近三分之一(968.1 万[903.5-1040.3])居住在南亚。
本研究表明,衡量有效覆盖及其在支持所有人获得更好健康结果方面的作用的效用,这是 UHC 的最终目标及其实现。除非在非传染性疾病方面采取协调一致的行动,各国能够更好地将卫生支出转化为改善的绩效,否则全球加快推进 UHC 服务覆盖的雄心壮志不太可能实现。关注有效覆盖,并考虑世界不断变化的健康需求,为更好地了解所有人群距离或离受益于 UHC 还有多远奠定了基础。
比尔及梅琳达·盖茨基金会。