Ayandipo Omobolaji O, Ogun Gabriel O, Adepoju Olalekan J, Fatunla Ebenezer O, Afolabi Adefemi O, Osuala Peter C, Ogundiran Temidayo O
Department of Surgery, College of Medicine, University of Ibadan and University College Hospital, Ibadan, Nigeria.
https://orcid.org/0000-0002-6806-8015.
Ecancermedicalscience. 2020 Aug 5;14:1084. doi: 10.3332/ecancer.2020.1084. eCollection 2020.
Oncologic surgical extirpation, the mainstay of loco-regional disease control in breast cancer, is aimed at achieving negative margins and lymph node clearance. Even though axillary lymph nodal metastasis is a critical index of prognostication, establishing the impact of lymph node ratio (LNR) and adequate surgical margins on disease-specific survivorship would be key to achieving longer survival. This study examines the prognostic role of pN (lymph nodes positive for malignancy), LNR and resection margin on breast cancer survival in a tertiary hospital in Ibadan, Nigeria.
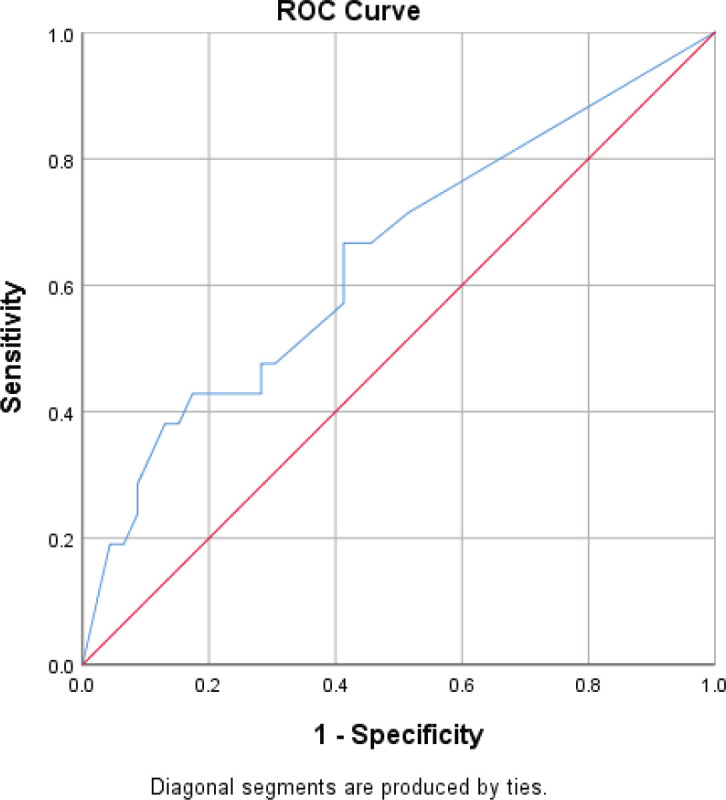
We conducted a longitudinal cohort study of 225 patients with breast carcinoma, documented clinico-pathologic parameters and 5-year follow up outcomes - distant metastasis and survival. Chi-square test and logistic regression analysis were used to evaluate the interaction of resection margin and proportion of metastatic lymph nodes with patients' survival. The receiver operating characteristic curve was plotted to determine the proportion of metastatic lymph nodes which predicted survival. The survival analysis was done using Kaplan-Meier method.
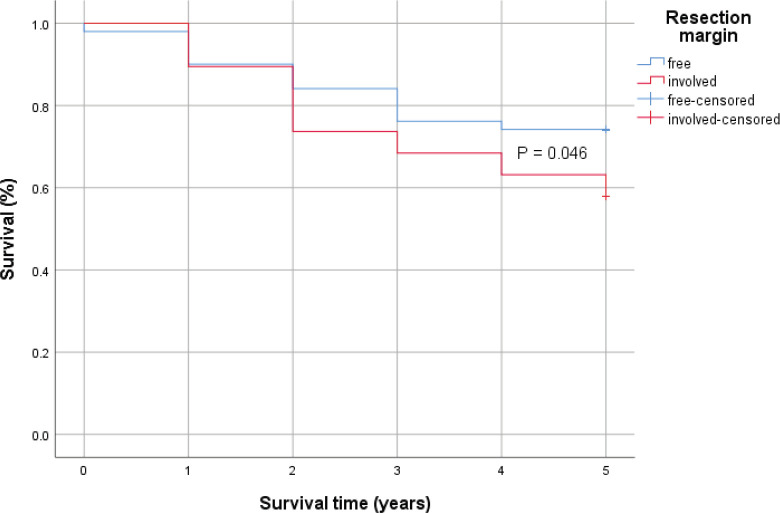
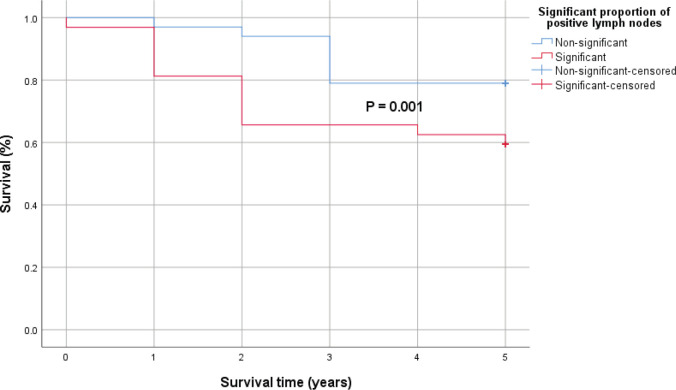
Sixty (26.7%) patients of the patients had positive resection margins, with the most common immuno-histochemical type being Lumina A. 110 (49%) patients had more than 10 axillary lymph nodes harvested. The mean age was 48.6 ± 11.8 years. Tumour size (p = 0.018), histological type ( = 0.015), grade ( = 0.006), resection margin ( = 0.023), number of harvested nodes ( < 0.01), number of metastatic nodes ( < 0.001) and loco-regional recurrence ( < 0.01) are associated with survival. The overall 5-year survival was 65.3%.
Unfavourable survival outcomes following breast cancer treatment is multifactorial, including the challenges faced in the multimodal treatment protocol received by our patients.
肿瘤外科切除是乳腺癌局部区域疾病控制的主要手段,旨在实现切缘阴性和淋巴结清扫。尽管腋窝淋巴结转移是预后的关键指标,但确定淋巴结比率(LNR)和足够的手术切缘对疾病特异性生存率的影响将是实现更长生存期的关键。本研究在尼日利亚伊巴丹的一家三级医院中,探讨了pN(恶性淋巴结阳性)、LNR和手术切缘对乳腺癌生存的预后作用。
我们对225例乳腺癌患者进行了纵向队列研究,记录了临床病理参数和5年随访结果——远处转移和生存情况。采用卡方检验和逻辑回归分析来评估手术切缘和转移淋巴结比例与患者生存的相互作用。绘制受试者工作特征曲线以确定预测生存的转移淋巴结比例。使用Kaplan-Meier方法进行生存分析。
60例(26.7%)患者切缘阳性,最常见的免疫组织化学类型为Lumina A。110例(49%)患者切除了10个以上腋窝淋巴结。平均年龄为48.6±11.8岁。肿瘤大小(p = 0.018)、组织学类型(= 0.015)、分级(= 0.006)、手术切缘(= 0.023)、切除淋巴结数量(< 0.01)、转移淋巴结数量(< 0.001)和局部区域复发(< 0.01)与生存相关。总体5年生存率为65.3%。
乳腺癌治疗后不良的生存结果是多因素的,包括我们的患者在接受多模式治疗方案时面临的挑战。