BMC Pediatr. 2020 Sep 1;20(1):413. doi: 10.1186/s12887-020-02293-5.
India introduced rotavirus vaccines (RVV, monovalent, Rotavac™ and pentavalent, Rotasiil™) in April 2016 with 6, 10 and 14 weeks schedule and expanded countrywide in phases. We describe the epidemiology of intussusception among children aged 2-23 months in India.
The prospective surveillance at 19 nationally representative sentinel hospitals from four regions recruited children with intussusception from April 2016 to September 2017. Data on sociodemography, immunization, clinical, treatment and outcome were collected. Along with descriptive analysis, key parameters between four regions were compared using Chi-Square/Fisher's exact/Mann-Whitney U/Kruskal-Wallis tests. The pre- and post-RVV periods were compared to estimate the risk ratios.
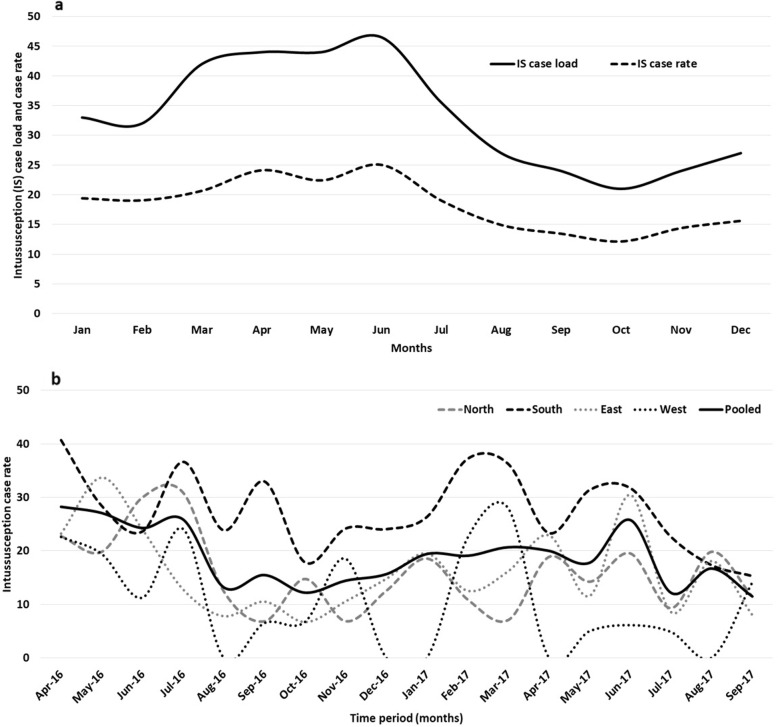
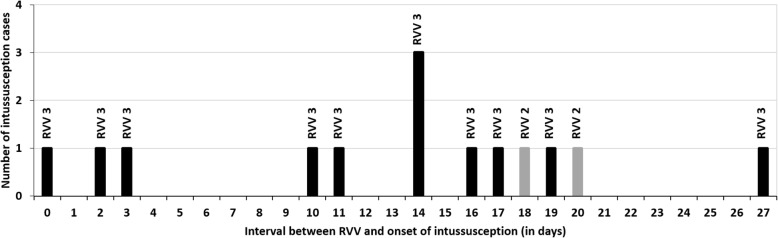
Six hundred twenty-one children with intussusception from South (n = 262), East (n = 190), North (n = 136) and West (n = 33) regions were recruited. Majority (n = 465, 74.8%) were infants (40.0% aged 4-7 months) with median age 8 months (IQR 5, 13 months), predominantly males (n = 408, 65.7%) and half (n = 311, 50.0%) occurred during March-June months. A shorter interval between weaning and intussusception was observed for ragi based food (median 1 month, IQR 0-4.2 months) compared to rice (median 4 months, IQR 1-9 months) and wheat (median 3 months, IQR 1-7 months) based food (p < 0.01). Abdominal pain or excessive crying (82.8%), vomiting (72.6%), and bloody stool (58.1%) were the leading symptoms. Classical triad (abdominal pain, vomiting and bloody stool) was observed in 34.8% cases (24.4 to 45.8% across regions). 95.3% of the cases were diagnosed by ultrasound. 49.3% (10.5 to 82.4% across regions) cases were managed by reduction, 39.5% (11.5 to 71.1% across regions) cases underwent surgery and 11.1% spontaneously resolved. Eleven (1.8%) cases died. 89.1% cases met Brighton criteria level 1 and 7.6% met Level 2. RVV was received by 12 cases within 1-21 days prior to intussusception. No increase in case load (RR = 0.44; 95% CI 0.22-1.18) or case ratio (RR = 0.5; 95% CI 0.3-1.2) was observed after RVV introduction in select sites.
Intussusception cases were observed across all sites, although there were variations in cases, presentation and mode of management. The high case load age coincided with age of the RVV third dose. The association with ragi based weaning food in intussusception needs further evaluation.
印度于2016年4月引入轮状病毒疫苗(RVV,单价疫苗Rotavac™和五价疫苗Rotasiil™),接种程序为6周、10周和14周龄,并分阶段在全国范围内推广。我们描述了印度2至23个月龄儿童肠套叠的流行病学情况。
在来自四个地区的19家具有全国代表性的哨点医院进行前瞻性监测,招募2016年4月至2017年9月期间患肠套叠的儿童。收集社会人口统计学、免疫接种、临床、治疗及转归等方面的数据。除描述性分析外,还使用卡方检验/费舍尔精确检验/曼-惠特尼U检验/克鲁斯卡尔-沃利斯检验对四个地区之间的关键参数进行比较。比较轮状病毒疫苗接种前后两个时期以估计风险比。
招募了来自南部(n = 262)、东部(n = 190)、北部(n = 136)和西部(n = 33)地区的621例肠套叠儿童。大多数(n = 465,74.8%)为婴儿(4 - 7个月龄的占40.0%),中位年龄为8个月(四分位间距5,13个月),以男性为主(n = 408,65.7%),半数(n = 311,50.0%)病例发生在3 - 6月。与以大米(中位时间4个月,四分位间距1 - 9个月)和小麦(中位时间3个月,四分位间距1 - 7个月)为基础的食物相比,食用基于拉吉的食物与肠套叠之间的间隔时间较短(中位时间1个月,四分位间距0 - 4.2个月)(p < 0.01)。腹痛或哭闹过度(82.8%)、呕吐(72.6%)和血便(58.1%)是主要症状。34.8%的病例出现典型三联征(腹痛、呕吐和血便)(各地区为24.4%至45.8%)。95.3%的病例通过超声诊断。49.3%的病例(各地区为10.5%至82.4%)采用复位治疗,39.5%的病例(各地区为11.5%至71.1%)接受了手术,11.1%的病例自行缓解。11例(1.8%)死亡。89.1%的病例符合布莱顿标准1级,7.6%的病例符合2级。12例在肠套叠发生前1至21天内接种了轮状病毒疫苗。在选定地点引入轮状病毒疫苗后,未观察到病例数增加(风险比=0.44;95%置信区间0.22 - 1.18)或病例比例增加(风险比=0.5;95%置信区间0.3 - 1.2)。
尽管在病例、表现和治疗方式上存在差异,但在所有地点均观察到肠套叠病例。病例数高峰年龄与轮状病毒疫苗第三剂接种年龄一致。肠套叠与基于拉吉的断奶食品之间的关联需要进一步评估。