Matheson Center for Health Care Studies, the University of Utah, Salt Lake City.
Division of Infectious Disease, the University of Utah School of Medicine, Salt Lake City.
JAMA Netw Open. 2020 Sep 1;3(9):e2015756. doi: 10.1001/jamanetworkopen.2020.15756.
Between 2 and 3.5 million people live with chronic hepatitis C virus (HCV) infection in the US, most of whom (approximately 75%) are not aware of their disease. Despite the availability of effective HCV treatment in the early stages of infection, HCV will result in thousands of deaths in the next decade in the US.
To investigate the cost-effectiveness of universal screening for all US adults aged 18 years or older for HCV in the US and of targeted screening of people who inject drugs.
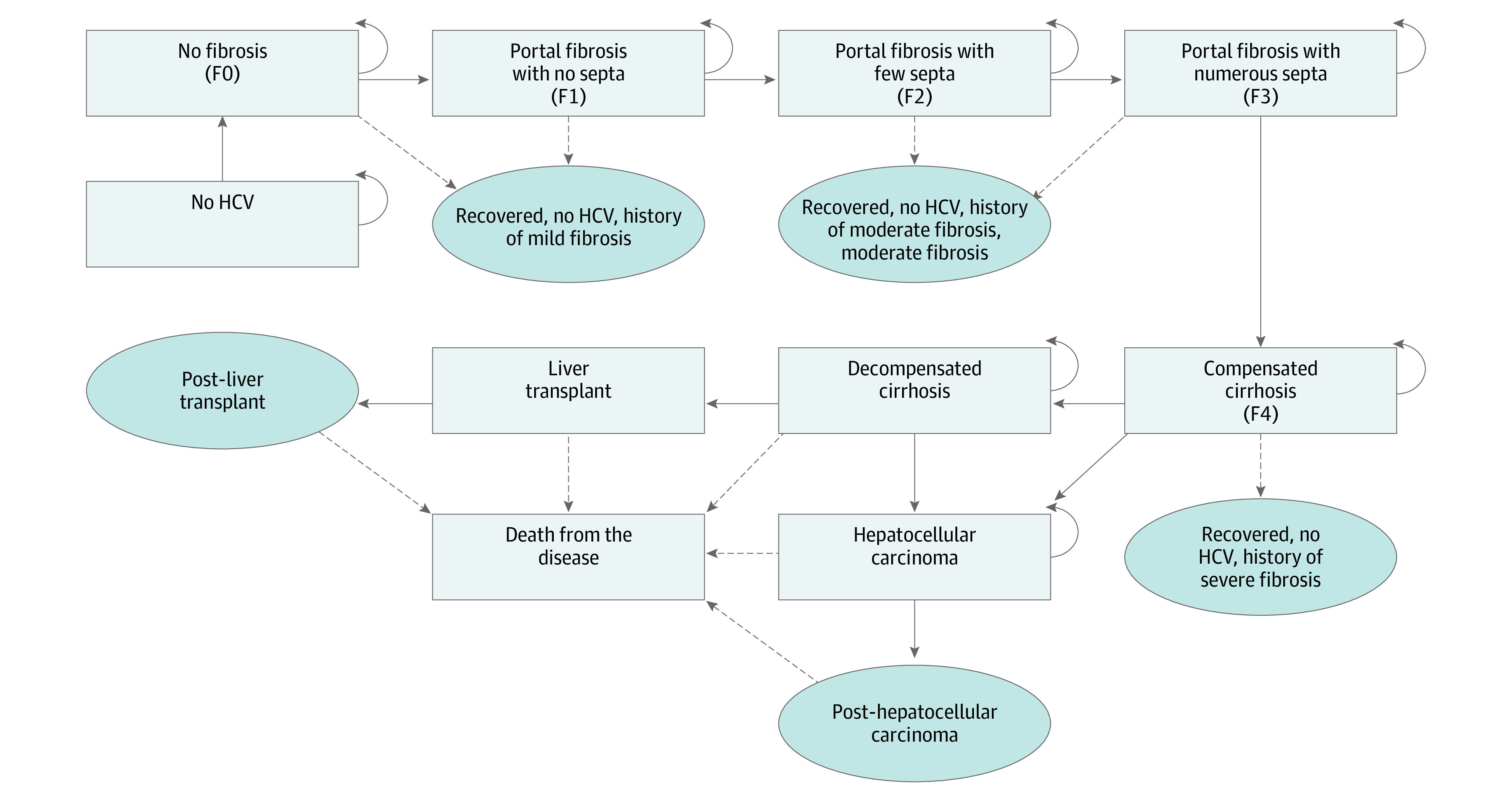
DESIGN, SETTING, AND PARTICIPANTS: This simulated economic evaluation used cohort analyses in a Markov model to perform a 10 000-participant Monte Carlo microsimulation trail to evaluate the cost-effectiveness of HCV screening programs, and compared screening programs targeting people who inject drugs with universal screening of US adults age 18 years or older. Data were analyzed in December 2019.
Cost per quality-adjusted life-year (QALY).
Cost per QALY gained.
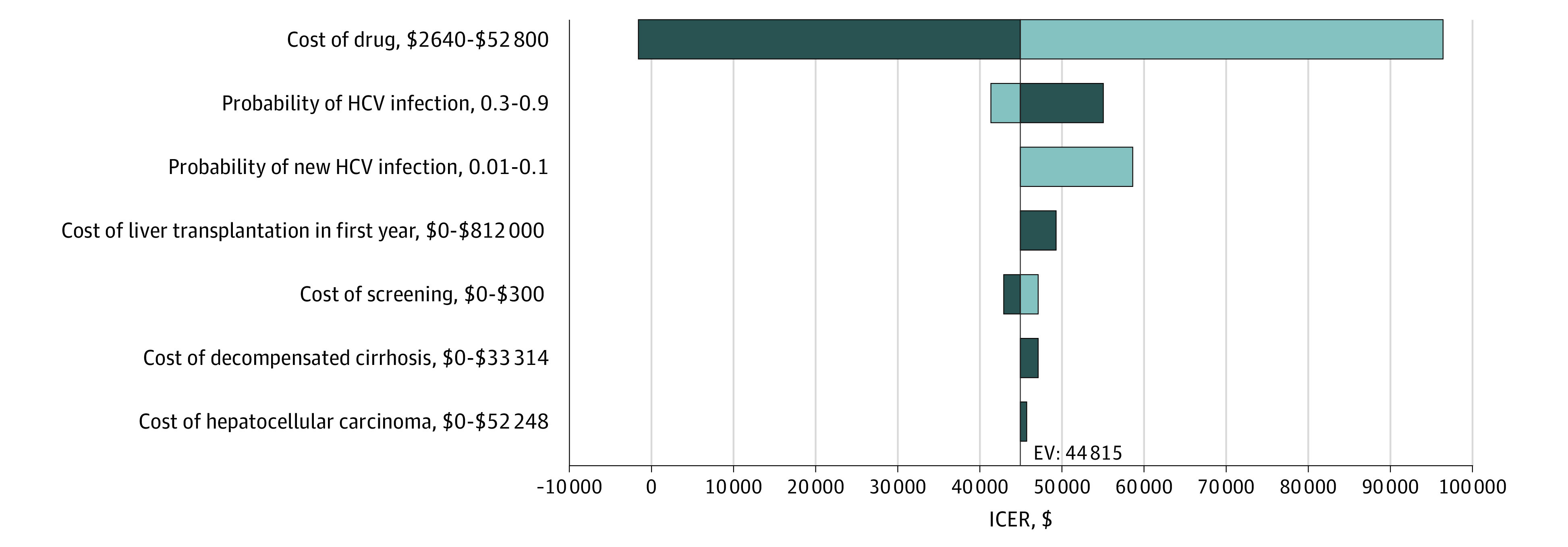
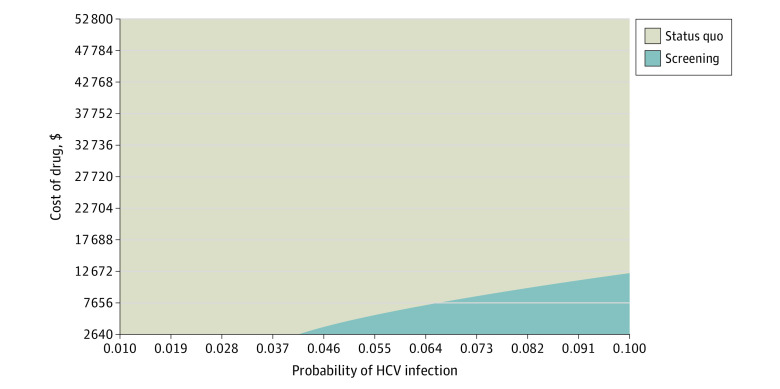
In a 10 000 Monte Carlo microsimulation trail that compared a baseline of individuals aged 40 years (men and women) and people who inject drugs in the US, screening and treatment for HCV were estimated to increase total costs by $10 457 per person and increase QALYs by 0.23 (approximately 3 months), providing an incremental cost-effectiveness ratio of $45 465 per QALY. Also, universal screening and treatment for HCV are estimated to increase total costs by $2845 per person and increase QALYs by 0.01, providing an incremental cost-effectiveness ratio of $291 277 per QALY.
The findings of this study suggest that HCV screening for people who inject drugs may be a cost-effective intervention to combat HCV infection in the US, which could potentially decrease the risk of untreated HCV infection and liver-related mortality.
在美国,有 200 万至 350 万人患有慢性丙型肝炎病毒 (HCV) 感染,其中大多数(约 75%)不知道自己患有这种疾病。尽管在 HCV 感染的早期阶段就可以进行有效的治疗,但在美国,在未来十年内,HCV 将导致数千人死亡。
研究在美国对所有 18 岁或以上的成年人进行 HCV 普遍筛查以及对注射毒品者进行目标筛查的成本效益。
设计、设置和参与者:本模拟经济评估使用队列分析和马尔可夫模型进行了 10000 名参与者的蒙特卡罗微模拟试验,以评估 HCV 筛查计划的成本效益,并将针对注射毒品者的筛查计划与美国成年人的普遍筛查进行比较。数据于 2019 年 12 月进行了分析。
每质量调整生命年 (QALY) 的成本。
每获得一个 QALY 的成本。
在一项对美国 40 岁人群(男女)和注射毒品者的 10000 个蒙特卡罗微模拟试验中,对 HCV 的筛查和治疗进行了比较,结果估计,每例患者的总成本将增加 10457 美元,增加 QALY 0.23(约 3 个月),增量成本效益比为每 QALY 45465 美元。此外,对 HCV 的普遍筛查和治疗估计将使每个人的总成本增加 2845 美元,并增加 0.01 的 QALY,增量成本效益比为每 QALY 291277 美元。
本研究结果表明,对注射毒品者进行 HCV 筛查可能是美国对抗 HCV 感染的一种具有成本效益的干预措施,这可能降低未治疗的 HCV 感染和与肝脏相关的死亡率的风险。