Fu Michael, Vedin Ola, Svennblad Bodil, Lampa Erik, Johansson Daniel, Dahlström Ulf, Lindmark Krister, Vasko Peter, Lundberg Anna, Costa-Scharplatz Madlaina, Lund Lars H
Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden.
ESC Heart Fail. 2020 Dec;7(6):3633-3643. doi: 10.1002/ehf2.12883. Epub 2020 Sep 3.
The aim of this study is to study the introduction of sacubitril/valsartan (sac/val) in Sweden with regards to regional differences, clinical characteristics, titration patterns, and determinants of use and discontinuation.
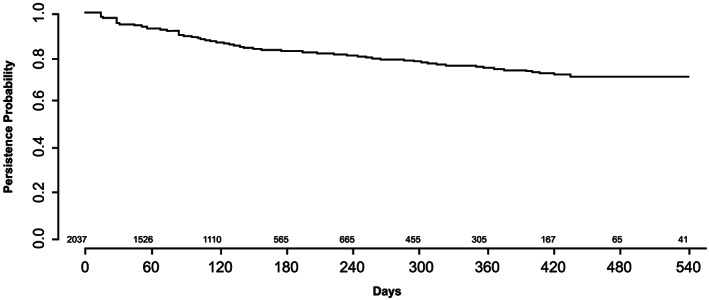
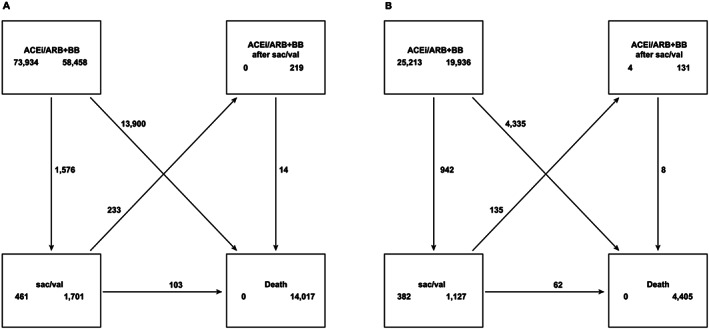
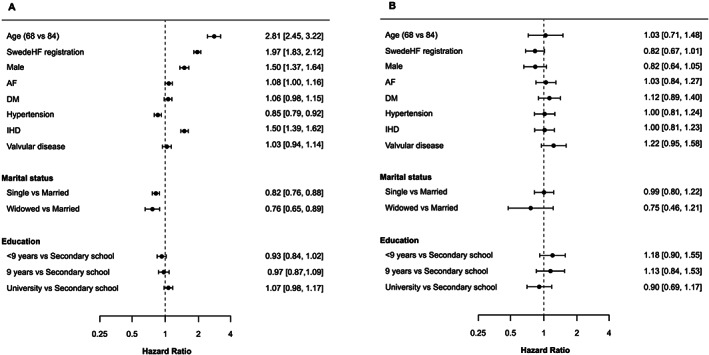
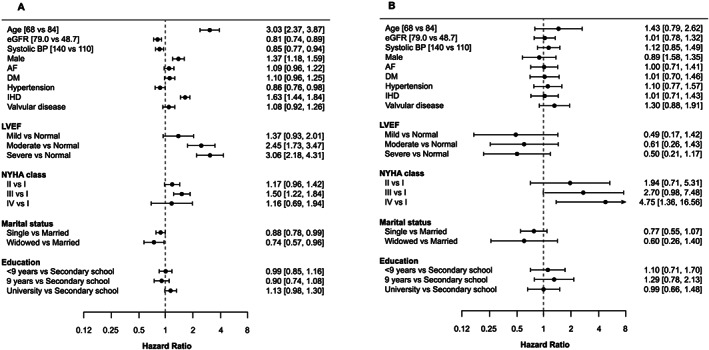
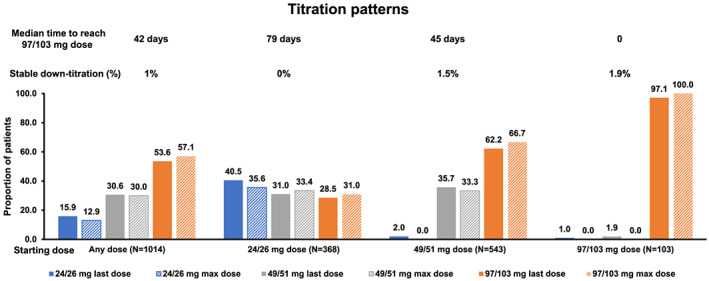
A national cohort of heart failure was defined from the Swedish Prescribed Drug Register and National Patient Register. A subcohort with additional data from the Swedish Heart Failure Registry (SwedeHF) was also studied. Cohorts were subdivided as per sac/val prescription and registration in SwedeHF. Median sac/val prescription rate was 20 per 100 000 inhabitants. Between April 2016 and December 2017, we identified 2037 patients with ≥1 sac/val prescription, of which 1144 (56%) were registered in SwedeHF. Overall, patients prescribed with sac/val were younger, more frequently male, and had less prior cardiovascular disease than non-sac/val patients. In SwedeHF subcohort, patients prescribed with sac/val had lower ejection fraction. Overall, younger age [hazard ratio 2.81 (95% confidence interval 2.45-3.22)], registration in SwedeHF [1.97 (1.83-2.12)], male gender [1.50 (1.37-1.64)], ischaemic heart disease [1.50 (1.39-1.62)], lower left ventricular ejection fraction [3.06 (2.18-4.31)], and New York Heart Association IV [1.50 (1.22-1.84)] were predictors for sac/val use. As initiation dose in the sac/val cohort, 38% received 24/26 mg, 54% 49/51 mg, and 9% 97/103 mg. Up-titration to the target dose was achieved in 57% of the overall cohort over a median follow-up of 6 months. The estimated treatment persistence for any dose at 360 days was 82%.
Implementation of sac/val in Sweden was slow and varied five-fold across different regions; younger age, male, SwedeHF registration, and ischaemic heart disease were among the independent predictors of receiving sac/val. Overall, treatment persistence and tolerability was high.
本研究旨在探讨沙库巴曲缬沙坦(沙库/缬)在瑞典的引入情况,涉及地区差异、临床特征、滴定模式以及使用和停药的决定因素。
从瑞典处方药登记册和国家患者登记册中确定了一个全国性的心力衰竭队列。还研究了一个从瑞典心力衰竭登记册(SwedeHF)获取额外数据的亚队列。根据SwedeHF中的沙库/缬处方和登记情况对队列进行细分。沙库/缬的中位处方率为每10万居民20例。在2016年4月至2017年12月期间,我们确定了2037例有≥1次沙库/缬处方的患者,其中1144例(56%)在SwedeHF中登记。总体而言,与未使用沙库/缬的患者相比,使用沙库/缬的患者更年轻,男性更常见,既往心血管疾病更少。在SwedeHF亚队列中,使用沙库/缬的患者射血分数更低。总体而言,年龄较小[风险比2.81(95%置信区间2.45 - 3.22)]、在SwedeHF中登记[1.97(1.83 - 2.12)]、男性[1.50(1.37 - 1.64)]、缺血性心脏病[1.50(1.39 - 1.62)]、较低的左心室射血分数[3.06(2.18 - 4.31)]和纽约心脏协会IV级[1.50(1.22 - 1.84)]是使用沙库/缬的预测因素。作为沙库/缬队列的起始剂量,38%的患者接受24/26毫克,54%接受49/51毫克,9%接受97/103毫克。在中位随访6个月期间,57%的总体队列患者滴定至目标剂量。360天时任何剂量的估计治疗持续率为82%。
沙库/缬在瑞典的实施进展缓慢,不同地区差异达五倍之多;年龄较小、男性、在SwedeHF中登记以及缺血性心脏病是接受沙库/缬的独立预测因素。总体而言,治疗持续率和耐受性较高。