Department of Cardiovascular Medicine, Mayo Clinic, MN, USA.
Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, MN, USA.
J Physiol. 2020 Dec;598(23):5379-5390. doi: 10.1113/JP280333. Epub 2020 Sep 23.
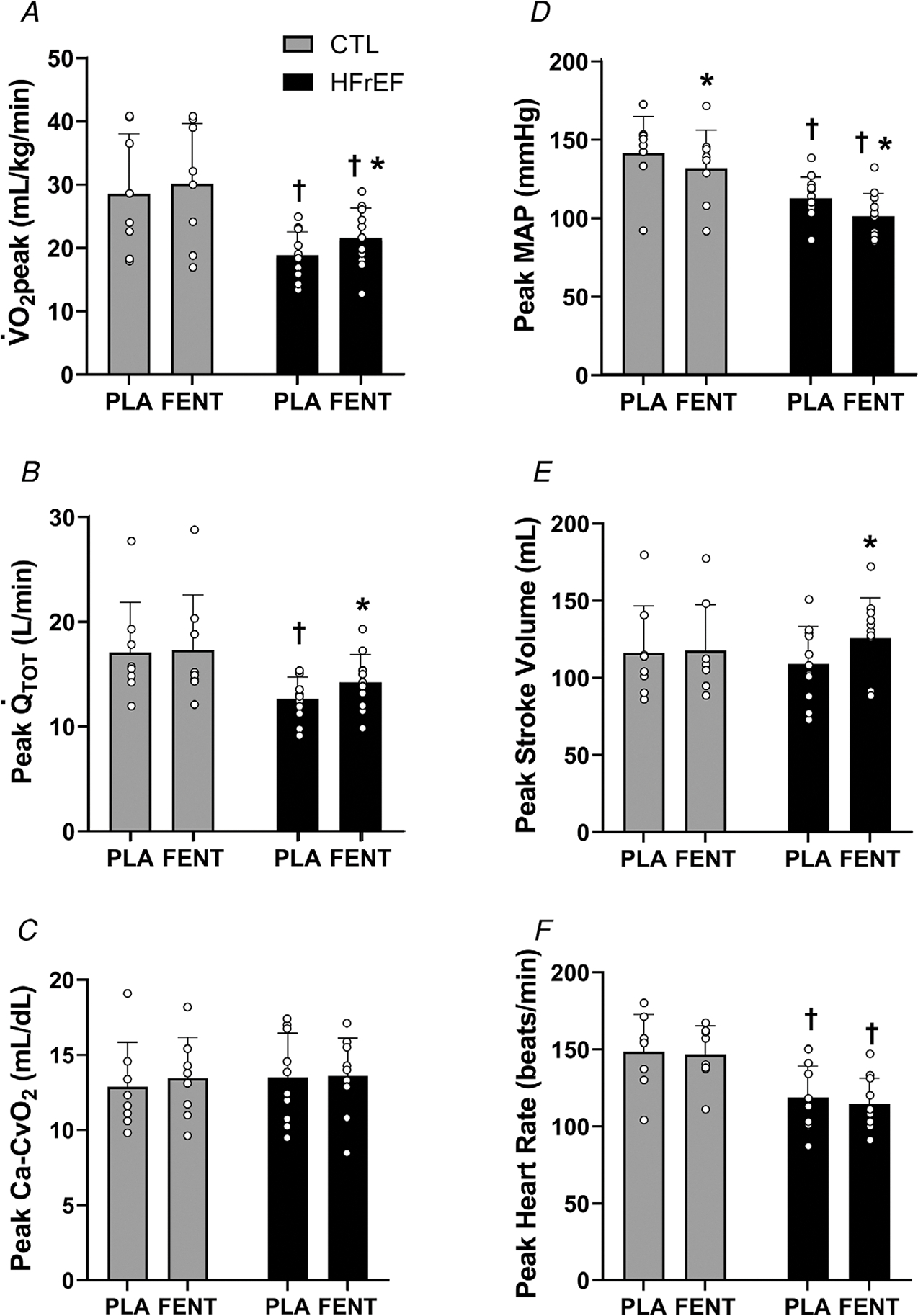
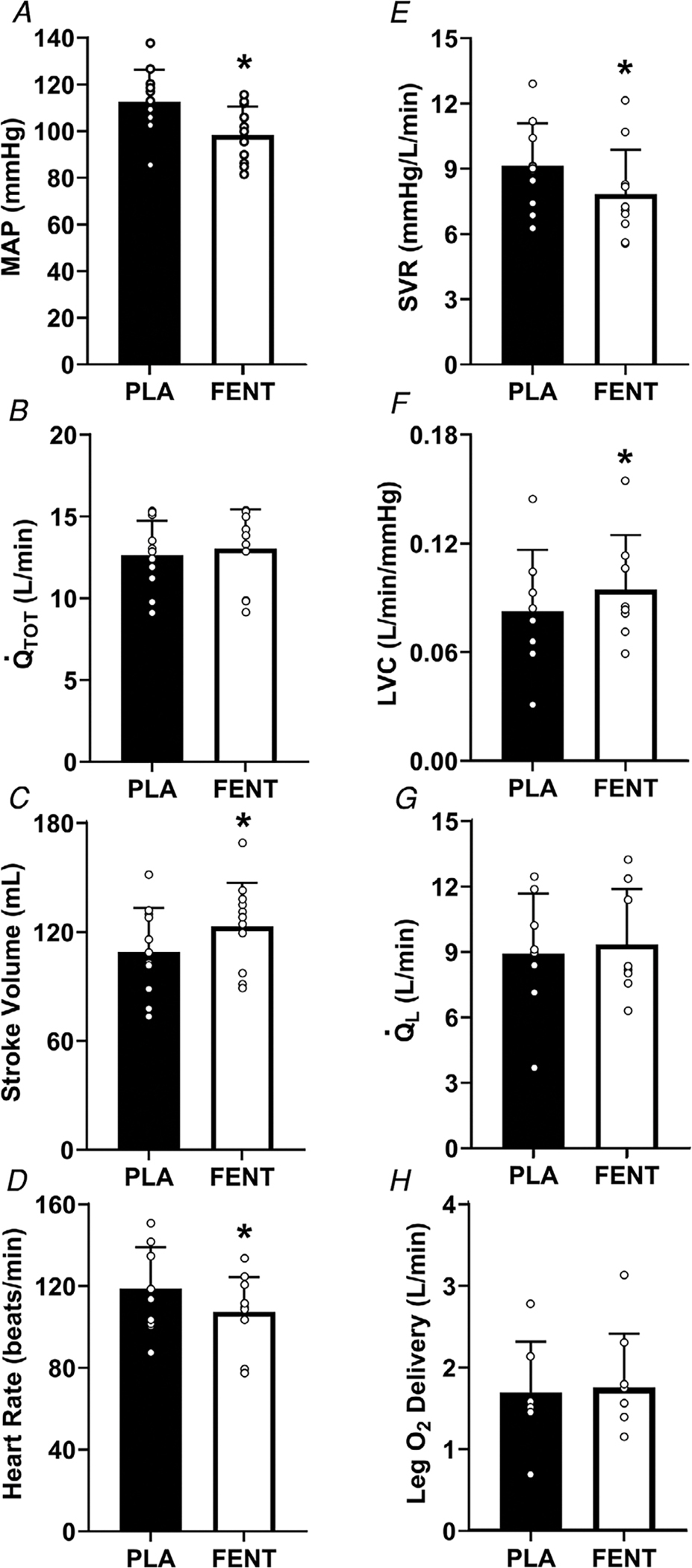
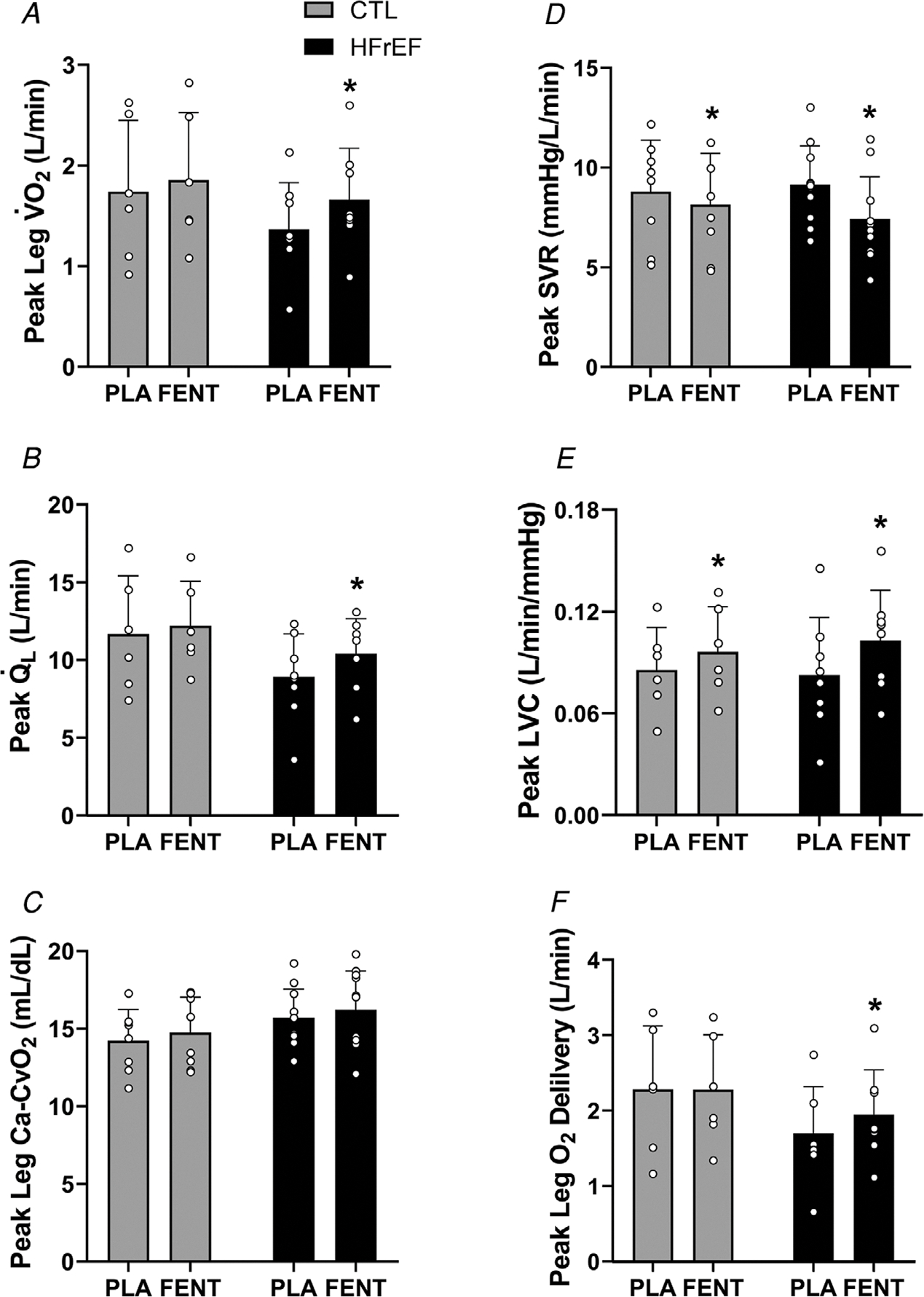
Heart failure patients with reduced ejection fraction (HFrEF) exhibit severe limitations in exercise capacity ( peak). One of the primary peripheral mechanisms suggested to underlie exercise intolerance in HFrEF is excessive locomotor muscle group III/IV afferent feedback; however, this has never been investigated in human heart failure. HFrEF patients and controls performed an incremental exercise test to volitional exhaustion to determine peak with lumbar intrathecal fentanyl or placebo. During exercise, cardiac output, leg blood flow and radial artery and femoral venous blood gases were measured. With fentanyl, compared with placebo, patients with HFrEF achieved a higher peak workload, peak, cardiac output, stroke volume and leg blood flow. These findings suggest that locomotor muscle group III/IV afferent feedback in HFrEF leads to increased systemic vascular resistance, which constrains stroke volume, cardiac output and O delivery thereby impairing peak and thus exercise capacity.
To better understand the underlying mechanisms contributing to exercise limitation in heart failure with reduced ejection fraction (HFrEF), we investigated the influence of locomotor muscle group III/IV afferent inhibition via lumbar intrathecal fentanyl on peak exercise capacity ( peak) and the contributory mechanisms. Eleven HFrEF patients and eight healthy matched controls were recruited. The participants performed an incremental exercise test to volitional exhaustion to determine peak with lumbar intrathecal fentanyl or placebo. During exercise, cardiac output and leg blood flow ( ) were measured via open-circuit acetylene wash-in technique and constant infusion thermodilution, respectively. Radial artery and femoral venous blood gases were measured. peak was 15% greater with fentanyl compared with placebo for HFrEF (P < 0.01), while no different in the controls. During peak exercise with fentanyl, cardiac output was 12% greater in HFrEF secondary to significant decreases in systemic vascular resistance and increases in stroke volume compared with placebo (all, P < 0.01). From placebo to fentanyl, leg , and O delivery were greater for HFrEF during peak exercise (all, P < 0.01), but not control. These findings indicate that locomotor muscle group III/IV afferent feedback in patients with HFrEF leads to increased systemic vascular resistance, which constrains stroke volume, cardiac output and O delivery, thereby impairing peak and thus exercise capacity. These findings have important clinical implications as peak is highly predictive of morbidity and mortality in HF.
射血分数降低的心力衰竭(HFrEF)患者表现出运动能力(峰值)的严重限制。被认为是 HFrEF 运动不耐受的主要外周机制之一是运动肌群 III/IV 传入反馈过度;然而,这在人类心力衰竭中从未被研究过。HFrEF 患者和对照组进行递增运动试验至自愿衰竭,以确定腰椎鞘内芬太尼或安慰剂的峰值。在运动过程中,测量心输出量、腿部血流量以及桡动脉和股静脉血气。与安慰剂相比,使用芬太尼时,HFrEF 患者达到更高的峰值工作量、峰值、心输出量、每搏量和腿部血流量。这些发现表明,HFrEF 中的运动肌群 III/IV 传入反馈导致全身血管阻力增加,从而限制每搏量、心输出量和 O 输送,从而损害峰值和运动能力。
为了更好地了解射血分数降低的心力衰竭(HFrEF)运动受限的潜在机制,我们通过腰椎鞘内芬太尼研究了运动肌群 III/IV 传入抑制对峰值运动能力(峰值)的影响和促成机制。招募了 11 名 HFrEF 患者和 8 名健康匹配的对照者。参与者进行递增运动试验至自愿衰竭,以确定腰椎鞘内芬太尼或安慰剂的峰值。在运动过程中,通过开路乙炔洗入技术和恒速输注热稀释法分别测量心输出量和腿部血流量()。测量桡动脉和股静脉血气。与安慰剂相比,HFrEF 患者使用芬太尼时峰值增加 15%(P<0.01),而对照组则无差异。在峰值运动时使用芬太尼,HFrEF 患者的心输出量增加 12%,这归因于全身血管阻力显著降低和每搏量增加(均 P<0.01)。与安慰剂相比,从芬太尼到安慰剂,HFrEF 患者在峰值运动时腿部血流量()、和 O 输送均增加(均 P<0.01),但对照组则无差异。这些发现表明,HFrEF 患者的运动肌群 III/IV 传入反馈导致全身血管阻力增加,从而限制了每搏量、心输出量和 O 输送,从而损害了峰值和运动能力。这些发现具有重要的临床意义,因为峰值是 HF 发病率和死亡率的高度预测指标。