Rijnstate, Arnhem, the Netherlands.
Cardiovascular Research Institute Maastricht, Maastricht, the Netherlands.
J Thromb Haemost. 2020 Dec;18(12):3280-3288. doi: 10.1111/jth.15081. Epub 2020 Sep 25.
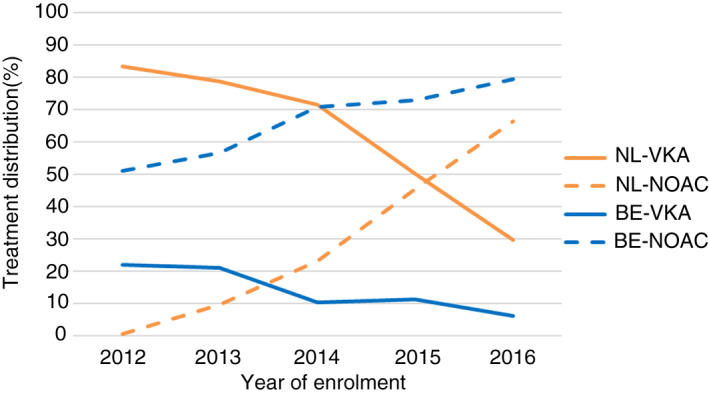
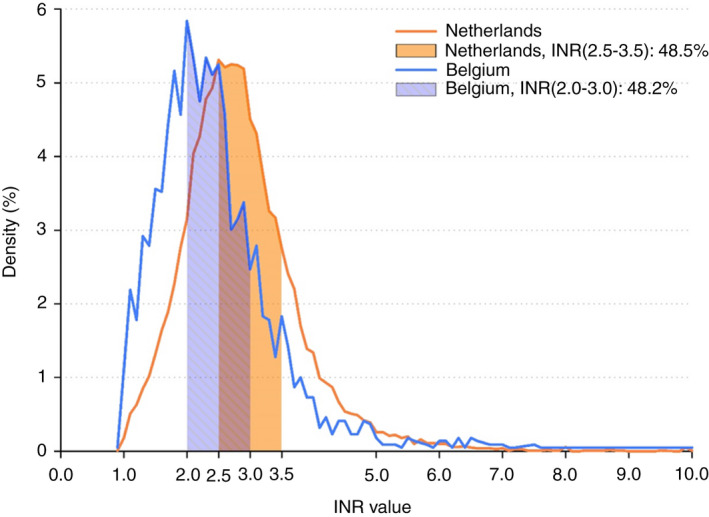
The uptake rate of non-vitamin K oral anticoagulants (NOAC) for the treatment of non-valvular atrial fibrillation (AF) was far lower in the Netherlands (NL) compared to Belgium (BE). Also, patients on VKA in NL were treated with a higher target international normalized ratio (INR) range of 2.5 to 3.5.
To explore the effect of these differences on thromboembolism (TE) and bleeding.
Data from the GARFIELD-AF registry was used. Patients with new-onset AF and ≥1 investigator-determined risk factor for stroke were included between 2010 and 2016. Event rates from 2 years of follow-up were used.
In NL and BE, 1186 and 1705 patients were included, respectively. Female sex (42.3% vs 42.2%), mean age (70.7 vs 71.3 years), CHA DS -VASc (3.1 vs 3.1), and HAS-BLED score (1.4 vs 1.5) were comparable between NL and BE. At diagnosis in NL vs BE, 72.1% vs 14.6% received vitamin K antagonists (VKA) and 17.8% vs 65.5% NOACs, varying greatly across cohorts. Mean INR was 2.9 (±1.0) and 2.4 (±1.0) in NL and BE, respectively. Event rates per 100 patient-years in NL and BE, respectively, of all-cause mortality (3.38 vs 3.90; hazard ratio [HR] 0.86, 95% confidence interval [CI] 0.65-1.15), ischemic stroke/TE (0.82 vs 0.72; HR 1.14, 95% CI 0.62-2.11), and major bleeding (2.06 vs 1.54; HR 1.33, 95% CI 0.89-1.99) did not differ significantly.
In GARFIELD-AF, despite similar characteristics, patients on anticoagulants were treated differently in NL and BE. Although the rate of major bleeding was 33% higher in NL, variations in bleeding, mortality, and TE rates were not statistically significant.
与比利时(BE)相比,荷兰(NL)使用非维生素 K 口服抗凝剂(NOAC)治疗非瓣膜性心房颤动(AF)的比例要低得多。此外,NL 中使用 VKA 的患者的目标国际标准化比值(INR)范围更高,为 2.5 至 3.5。
探讨这些差异对血栓栓塞(TE)和出血的影响。
使用 GARFIELD-AF 登记处的数据。纳入 2010 年至 2016 年期间新诊断为 AF 且至少有 1 项研究者确定的中风危险因素的患者。使用 2 年随访期间的事件发生率。
NL 和 BE 分别纳入 1186 例和 1705 例患者。女性比例(42.3% vs 42.2%)、平均年龄(70.7 岁 vs 71.3 岁)、CHA2DS2-VASc 评分(3.1 分 vs 3.1 分)和 HAS-BLED 评分(1.4 分 vs 1.5 分)在 NL 和 BE 之间无差异。NL 与 BE 相比,诊断时分别有 72.1%和 14.6%的患者接受维生素 K 拮抗剂(VKA)治疗,分别有 17.8%和 65.5%的患者接受非维生素 K 口服抗凝剂(NOAC)治疗,这些比例在不同队列之间差异很大。NL 和 BE 的平均 INR 分别为 2.9(±1.0)和 2.4(±1.0)。NL 和 BE 的全因死亡率(3.38 比 3.90;风险比 [HR] 0.86,95%置信区间 [CI] 0.65-1.15)、缺血性中风/TE(0.82 比 0.72;HR 1.14,95% CI 0.62-2.11)和大出血(2.06 比 1.54;HR 1.33,95% CI 0.89-1.99)的发生率每 100 患者年无显著差异。
在 GARFIELD-AF 中,尽管患者特征相似,但 NL 和 BE 对接受抗凝治疗的患者的治疗方式不同。尽管 NL 中大出血的发生率高 33%,但出血、死亡率和 TE 发生率的差异无统计学意义。