Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 17 Panjiayuannanli, Chaoyang District, Beijing, 100021, China.
Radiat Oncol. 2020 Sep 4;15(1):212. doi: 10.1186/s13014-020-01637-w.
To analyze the patterns of locoregional recurrence in breast cancer patients after mastectomy.
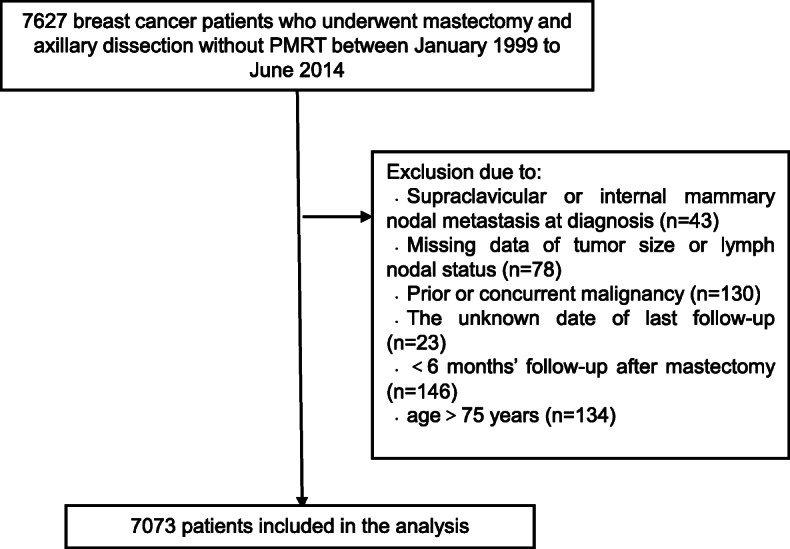
The retrospective study included 7073 women with breast cancer without post-mastectomy radiotherapy: 4604 (65.1%) had pT1-2 N0 disease (low risk); 2042 (28.9%), pT1-2 N1 (intermediate risk); and 427 (6.0%), pT3-4 and/or pN2-3, or pT1-2 N1 after neoadjuvant chemotherapy (high risk). The distribution of cumulative locoregional recurrence was analyzed. The local recurrence and regional recurrence rates were estimated by the Kaplan-Meier method, and differences were compared with the log-rank test. Multivariate analysis was performed using Cox logistic regression analysis.
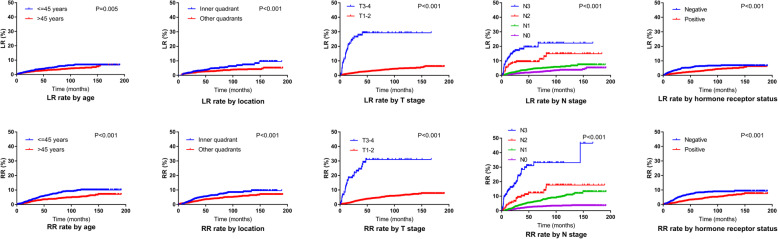
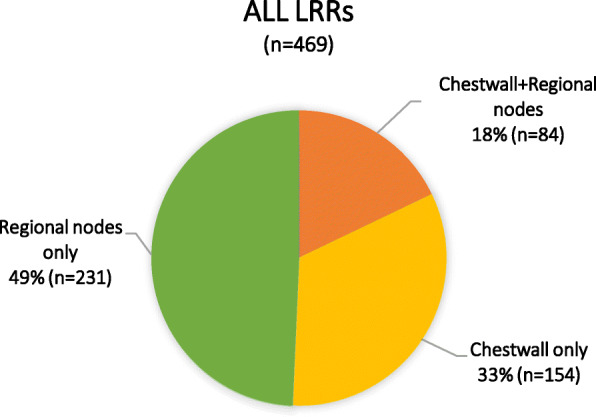
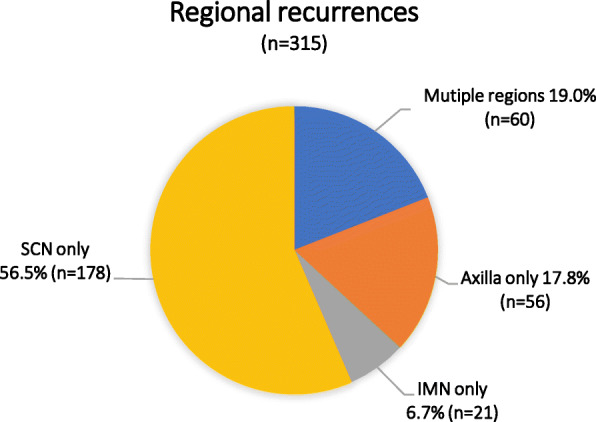
In the median follow-up of 63.0 months, 469 patients had locoregional recurrence: chest wall recurrence in 238 (50.7%) cases, supraclavicular/infraclavicular nodes in 236 (50.3%) cases, axilla in 92 (19.6%), and internal mammary nodes in 50 (10.7%) cases. The 5-year local recurrence and regional recurrence rates were 2.5 and 4.4%, respectively. Subgroup analysis of the three risk groups and five molecular subtypes (luminal A, luminal B-Her2 negative, luminal B-Her2 positive, Her2-enriched, and triple negative) also showed that the chest wall and supraclavicular/infraclavicular nodes were the most common recurrence sites. Age, tumor location, T stage, N stage, and hormone receptor status were independent prognostic factors for both local recurrence and regional recurrence (p < 0.05).
The chest wall and supraclavicular/infraclavicular nodes are common sites of locoregional recurrence in breast cancer, irrespective of disease stage or molecular subtype, and the prognostic factors for local recurrence and regional recurrence are similar. Therefore, chest wall and supraclavicular/infraclavicular nodes irradiation should always be considered in post-mastectomy radiotherapy.
分析乳腺癌患者乳房切除术后局部区域复发的模式。
本回顾性研究纳入了 7073 例未接受乳房切除术后放疗的乳腺癌患者:4604 例(65.1%)为 pT1-2N0 疾病(低危);2042 例(28.9%)为 pT1-2N1(中危);427 例(6.0%)为 pT3-4 和/或 pN2-3,或新辅助化疗后 pT1-2N1(高危)。分析了累积局部区域复发的分布情况。采用 Kaplan-Meier 法估计局部复发和区域复发率,并采用对数秩检验比较差异。采用 Cox 逻辑回归分析进行多变量分析。
在中位随访 63.0 个月时,469 例患者出现局部区域复发:胸壁复发 238 例(50.7%),锁骨上/锁骨下淋巴结复发 236 例(50.3%),腋窝复发 92 例(19.6%),内乳淋巴结复发 50 例(10.7%)。5 年局部复发和区域复发率分别为 2.5%和 4.4%。对三组风险组和五种分子亚型(管腔 A、管腔 B-Her2 阴性、管腔 B-Her2 阳性、Her2 富集型和三阴性)的亚组分析也表明,胸壁和锁骨上/锁骨下淋巴结是最常见的复发部位。年龄、肿瘤位置、T 分期、N 分期和激素受体状态是局部复发和区域复发的独立预后因素(p<0.05)。
无论疾病阶段或分子亚型如何,乳腺癌患者局部区域复发的常见部位为胸壁和锁骨上/锁骨下淋巴结,局部复发和区域复发的预后因素相似。因此,乳房切除术后放疗时应始终考虑胸壁和锁骨上/锁骨下淋巴结照射。