From the Department of Neurology (A.L.F., V.W.C., S.F., M.B.M., A.M.B., V.B., Y.T., P.K., Y.C., J.H., J.-M.L.), Mallinckrodt Institute of Radiology (A.L.F., J.-M.L., H.A.), Department of Ophthalmology (M.G.G.), and Department of Medicine (M.B., M.K.L., D.H., J.J.M., J.P.A.), Division of Rheumatology, Washington University School of Medicine, St. Louis, MO; Department of Radiology (D.L.), The Johns Hopkins University School of Medicine, Baltimore, MD; and Department of Neurology (J.C.J.), Icahn School of Medicine at Mount Sinai, New York, NY.
Neurology. 2020 Oct 6;95(14):e1918-e1931. doi: 10.1212/WNL.0000000000010659. Epub 2020 Sep 4.
To characterize lesion evolution and neurodegeneration in retinal vasculopathy with cerebral leukoencephalopathy and systemic manifestations (RVCL-S) using multimodal MRI.
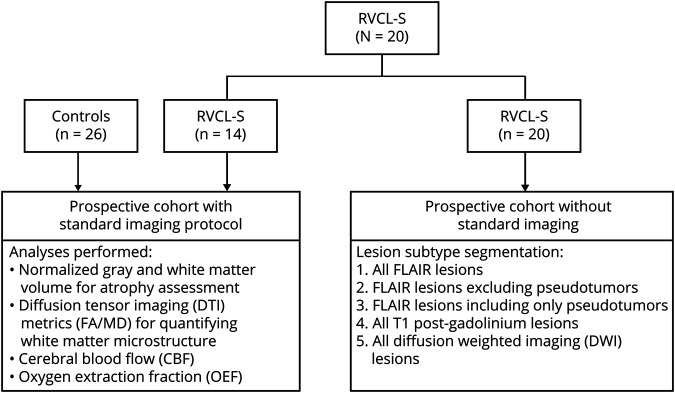
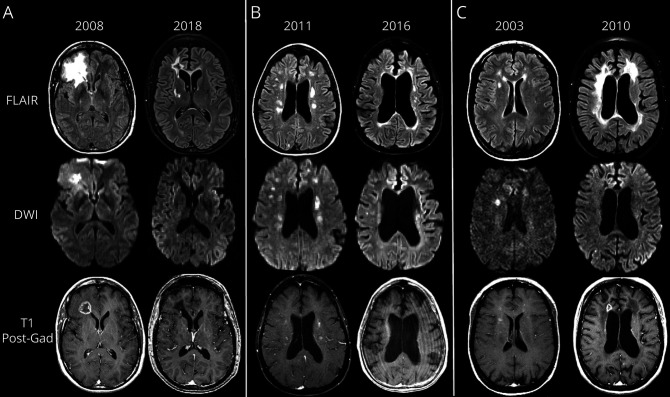
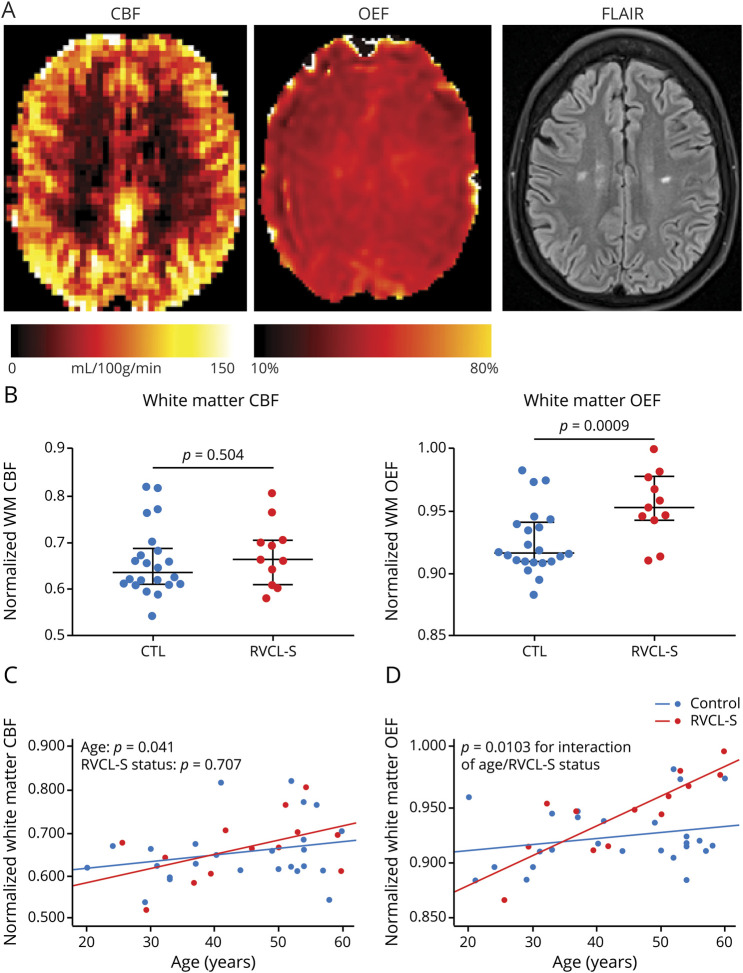
We prospectively performed MRI and cognitive testing in RVCL-S and healthy control cohorts. Gray and white matter volume and disruption of white matter microstructure were quantified. Asymmetric spin echo acquisition permitted voxel-wise oxygen extraction fraction (OEF) calculation as an in vivo marker of microvascular ischemia. The RVCL-S cohort was included in a longitudinal analysis of lesion subtypes in which hyperintense lesions on fluid-attenuated inversion recovery (FLAIR), T1-postgadolinium, and diffusion-weighted imaging were delineated and quantified volumetrically.
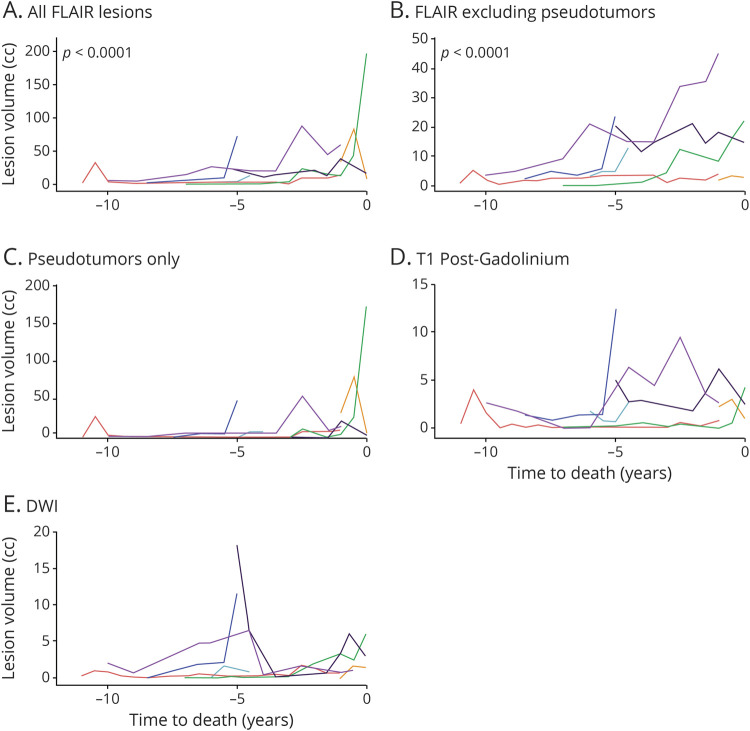
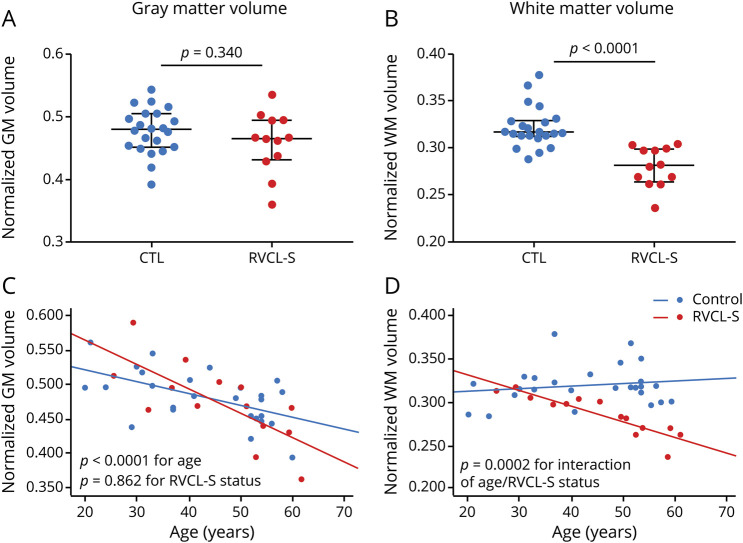
Twenty individuals with RVCL-S and 26 controls were enrolled. White matter volume and microstructure declined faster in those with RVCL-S compared to controls. White matter atrophy in RVCL-S was highly linear (ρ = -0.908, < 0.0001). Normalized OEF was elevated in RVCL-S and increased with disease duration. Multiple cognitive domains, specifically those measuring working memory and processing speed, were impaired in RVCL-S. Lesion volumes, regardless of subtype, progressed/regressed with high variability as a function of age, while FLAIR lesion burden increased near time to death ( < 0.001).
RVCL-S is a monogenic microvasculopathy affecting predominantly the white matter with regard to atrophy and cognitive impairment. White matter volumes in RVCL-S declined linearly, providing a potential metric against which to test the efficacy of future therapies. Progressive elevation of white matter OEF suggests that microvascular ischemia may underlie neurodegeneration in RVCL-S.
使用多模态 MRI 描绘视网膜血管病变伴脑白质病和全身表现(RVCL-S)中的病变演变和神经退行性变。
我们前瞻性地对 RVCL-S 和健康对照组进行 MRI 和认知测试。量化灰质和白质体积以及白质微观结构的破坏。不对称的自旋回波采集允许计算每个体素的氧提取分数(OEF),作为微血管缺血的体内标志物。RVCL-S 队列被纳入病变亚型的纵向分析中,其中对液体衰减反转恢复(FLAIR)、T1 后钆增强和弥散加权成像上的高信号病变进行描绘和量化体积。
共纳入 20 名 RVCL-S 患者和 26 名对照者。与对照组相比,RVCL-S 患者的白质体积和微观结构下降更快。RVCL-S 中的白质萎缩呈高度线性(ρ=-0.908,<0.0001)。RVCL-S 中的正常化 OEF 升高,并随疾病持续时间增加而增加。多个认知领域,特别是测量工作记忆和处理速度的领域,在 RVCL-S 中受损。无论病变亚型如何,病变体积都以高变异性随年龄进展/消退,而 FLAIR 病变负担在接近死亡时间时增加(<0.001)。
RVCL-S 是一种主要影响白质的单基因微血管病,表现为萎缩和认知障碍。RVCL-S 的白质体积呈线性下降,为未来治疗效果提供了潜在的衡量标准。白质 OEF 的逐渐升高提示微血管缺血可能是 RVCL-S 中神经退行性变的基础。