Division of Cardiology University of Toronto Toronto Canada.
Department of Neurology Boston University School of Medicine Boston MA.
J Am Heart Assoc. 2020 Sep 15;9(18):e014711. doi: 10.1161/JAHA.119.014711. Epub 2020 Sep 6.
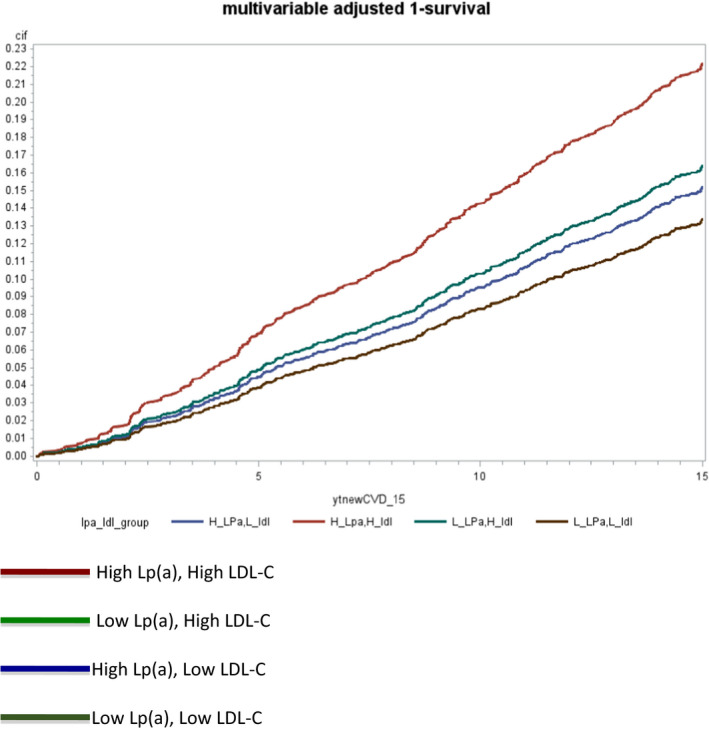
Background Elevated lipoprotein(a) is a well-established risk factor for atherosclerotic vascular disease but is not measured in routine clinical care. Screening of high lipoprotein(a) in individuals with moderate elevations of low-density lipoprotein cholesterol (LDL-C) may identify individuals at high risk of cardiovascular disease. Methods and Results We examined 2606 Framingham Offspring participants (median age, 54 years; 45% men) prospectively with a median follow-up of 15 years (n=392 incident cardiovascular events). Individuals with higher (≥100 nmol/L) versus lower lipoprotein(a) were divided into groups based on LDL-C <135 mg/dL versus ≥135 mg/dL. In Cox models, after adjustment for known risk factors, high lipoprotein(a) (≥100 nmol/L) and LDL-C ≥135 mg/dL were each significant predictors of cardiovascular disease (LDL-C ≥135 mg/dL: hazard ratio [HR], 1.34; 95% CI, 1.09-1.64; =0.006; high lipoprotein (a): HR, 1.31; 95% CI, 1.03-1.66; =0.026). Across the groups of high/low lipoprotein (a) and LDL-C ≥135 mg/dL or <135 mg/dL, the absolute cardiovascular disease risks at 15 years were 22.6% (high lipoprotein(a)/LDL-C ≥135 mg/dL, n=248), 17.3% (low lipoprotein(a)/LDL-C ≥135 mg/dL, n=758), 12.7% (high lipoprotein(a)/LDL-C <135 mg/dL, n=275) and 11.5% (low lipoprotein(a)/LDL-C <135 mg/dL, n=1328, reference group). Among individuals with LDL-C ≥135 mg/dL, those with high lipoprotein(a) had a 43% higher risk (HR, 1.43; 95% CI, 1.05-1.97; =0.02). Presence of high lipoprotein(a) with moderate LDL-C levels (135-159 mg/dL) yielded absolute risks equivalent to those with LDL-C ≥160 mg/dL (23.5%, 95% CI, 17.4%-31.3%; and 20.7%, 95% CI, 16.8%-25.3%, respectively). Conclusions Concomitant elevation of LDL-C ≥135 mg/dL and lipoprotein(a) ≥100 nmol/L is associated with a high absolute risk of incident cardiovascular disease. lipoprotein(a) measurement in individuals with moderate elevations in LDL-C, who do not otherwise meet criteria for statins, may identify individuals at high cardiovascular risk.
脂蛋白(a)升高是动脉粥样硬化性血管疾病的一个公认的危险因素,但在常规临床护理中并未测量。在低密度脂蛋白胆固醇 (LDL-C) 中度升高的个体中筛查高脂蛋白(a)可能会识别出心血管疾病风险较高的个体。
我们前瞻性地检查了 2606 名弗雷明汉后代参与者(中位年龄 54 岁;45%为男性),中位随访时间为 15 年(n=392 例心血管事件)。根据 LDL-C<135mg/dL 与≥135mg/dL 将脂蛋白(a)较高(≥100nmol/L)的个体分为两组。在 Cox 模型中,在校正了已知危险因素后,高脂蛋白(a)(≥100nmol/L)和 LDL-C≥135mg/dL 均为心血管疾病的显著预测因子(LDL-C≥135mg/dL:危险比 [HR],1.34;95%CI,1.09-1.64;=0.006;高脂蛋白(a):HR,1.31;95%CI,1.03-1.66;=0.026)。在高/低脂蛋白(a)和 LDL-C≥135mg/dL 或<135mg/dL 的组中,15 年的绝对心血管疾病风险分别为 22.6%(高脂蛋白(a)/LDL-C≥135mg/dL,n=248)、17.3%(低脂蛋白(a)/LDL-C≥135mg/dL,n=758)、12.7%(高脂蛋白(a)/LDL-C<135mg/dL,n=275)和 11.5%(低脂蛋白(a)/LDL-C<135mg/dL,n=1328,参考组)。在 LDL-C≥135mg/dL 的个体中,高脂蛋白(a)的风险增加 43%(HR,1.43;95%CI,1.05-1.97;=0.02)。中等 LDL-C 水平(135-159mg/dL)伴高脂蛋白(a)的绝对风险与 LDL-C≥160mg/dL 相当(23.5%,95%CI,17.4%-31.3%;和 20.7%,95%CI,16.8%-25.3%)。
同时升高 LDL-C≥135mg/dL 和脂蛋白(a)≥100nmol/L 与新发心血管疾病的高绝对风险相关。在 LDL-C 中度升高但不符合他汀类药物治疗标准的个体中测量脂蛋白(a),可能会识别出心血管风险较高的个体。