Key Laboratory of Pediatrics in Chongqing, Chongqing, 400014, China.
China International Science and Technology Cooperation base of Child development and Critical Disorders, Department of Children's Hospital of Chongqing Medical University of Education, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing, 400014, China.
BMC Infect Dis. 2020 Sep 9;20(1):665. doi: 10.1186/s12879-020-05257-3.
Pseudomonas aeruginosa (P. aeruginosa) is a major Gram-negative pathogen, which has been reported to result in high mortality. We aim to investigate the prognostic value and optimum cut-off point of time-to-positivity (TTP) of blood culture in children with P. aeruginosa bacteremia.
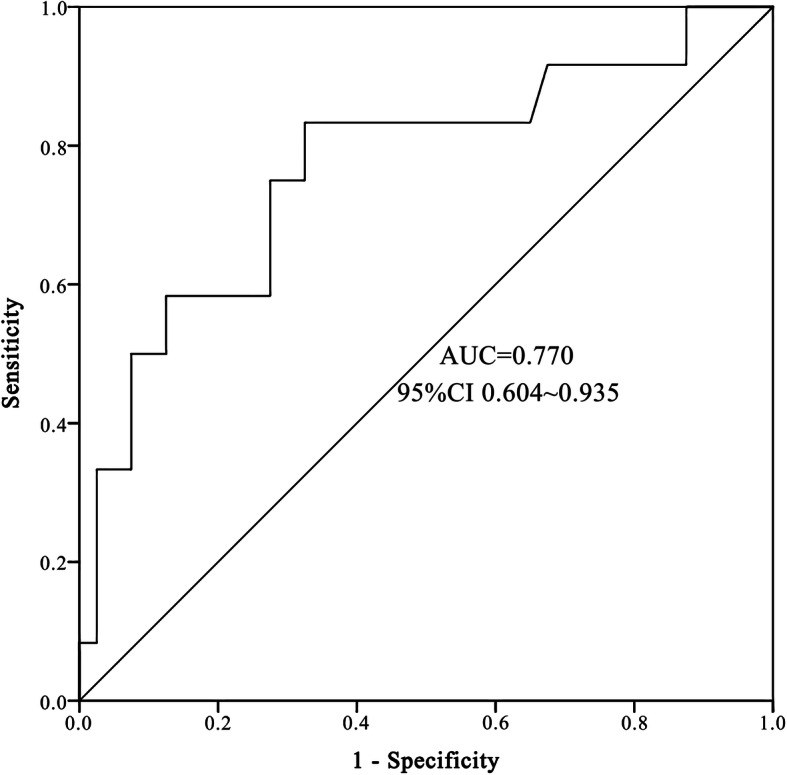
From August 2014 to November 2018, we enrolled the inpatients with P. aeruginosa bacteremia in a 1500-bed tertiary teaching hospital in Chongqing, China retrospectively. Receiver operating characteristic (ROC) analysis was used to determine the optimum cut-off point of TTP, and logistic regression were employed to explore the risk factors for in-hospital mortality and septic shock.
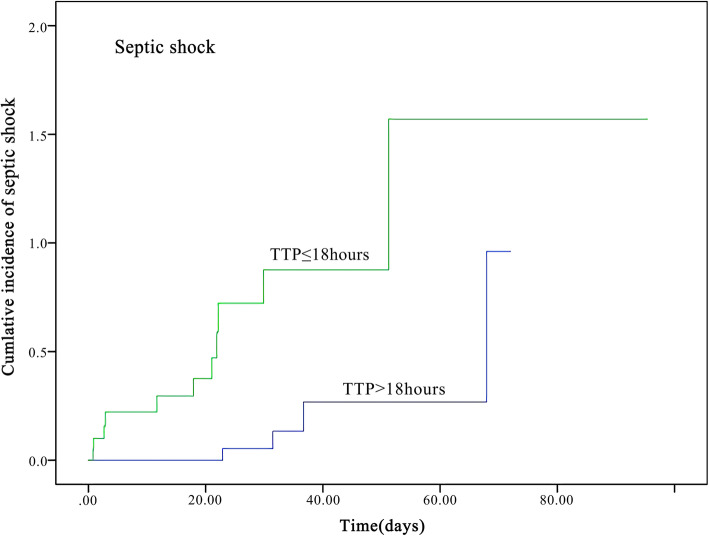
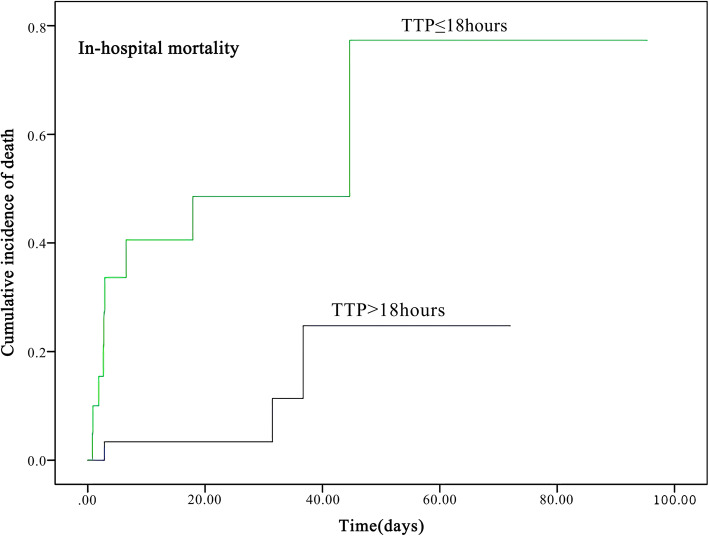
Totally, 52 children with P. aeruginosa bacteremia were enrolled. The standard cut-off point of TTP was18 h. Early TTP (≤18 h) group patients had remarkably higher in-hospital mortality (42.9% vs 9.7%, P = 0.014), higher incidence of septic shock (52.4% vs12.9%, P = 0.06), higher Pitt bacteremia scores [3.00 (1.00-5.00) vs 1.00 (1.00-4.00), P = 0.046] and more intensive care unit admission (61.9% vs 22.6%, P = 0.008) when compared with late TTP (> 18 h) groups. Multivariate analysis indicated TTP ≤18 h, Pitt bacteremia scores ≥4 were the independent risk factors for in-hospital mortality (OR 5.88, 95%CI 1.21-21.96, P = 0.035; OR 4.95, 95%CI 1.26-27.50, P = 0.024; respectively). The independent risk factors for septic shock were as follows: TTP ≤18 h, Pitt bacteremia scores ≥4 and hypoalbuminemia (OR 6.30, 95%CI 1.18-33.77, P = 0.032; OR 8.15, 95%CI 1.15-42.43, P = 0.014; OR 6.46, 95% CI 1.19-33.19 P = 0.031; respectively).
Early TTP (≤18 hours) appeared to be associated with worse outcomes for P. aeruginosa bacteremia children.
铜绿假单胞菌(P. aeruginosa)是一种主要的革兰氏阴性病原体,已被报道可导致高死亡率。我们旨在研究血培养中铜绿假单胞菌菌血症的时间至阳性(TTP)的预后价值和最佳截断点。
我们回顾性地纳入了 2014 年 8 月至 2018 年 11 月在中国重庆一家拥有 1500 张床位的三级教学医院住院的铜绿假单胞菌菌血症患者。采用受试者工作特征(ROC)分析确定 TTP 的最佳截断点,采用逻辑回归探讨院内死亡率和感染性休克的危险因素。
共纳入 52 例铜绿假单胞菌菌血症患者。TTP 的标准截断点为 18 小时。早期 TTP(≤18 小时)组患者的院内死亡率显著更高(42.9% vs 9.7%,P=0.014),感染性休克发生率更高(52.4% vs 12.9%,P=0.06),Pitt 菌血症评分更高[3.00(1.00-5.00)vs 1.00(1.00-4.00),P=0.046],入住重症监护病房的比例更高(61.9% vs 22.6%,P=0.008)。与晚期 TTP(>18 小时)组相比。多变量分析表明 TTP≤18 小时、Pitt 菌血症评分≥4 是院内死亡率的独立危险因素(OR 5.88,95%CI 1.21-21.96,P=0.035;OR 4.95,95%CI 1.26-27.50,P=0.024;分别)。感染性休克的独立危险因素如下:TTP≤18 小时、Pitt 菌血症评分≥4 和低白蛋白血症(OR 6.30,95%CI 1.18-33.77,P=0.032;OR 8.15,95%CI 1.15-42.43,P=0.014;OR 6.46,95%CI 1.19-33.19,P=0.031;分别)。
早期 TTP(≤18 小时)似乎与铜绿假单胞菌菌血症患儿的不良结局相关。