Diabetes Complications Research Centre, School of Medicine, Conway Institute of Biomolecular and Biomedical Research, University College Dublin, Belfield, Dublin 4, Ireland.
Department of Endocrinology, St. Vincent's University Hospital, Elm Park, Dublin 4, Ireland.
Sci Rep. 2020 Sep 9;10(1):14852. doi: 10.1038/s41598-020-71684-6.
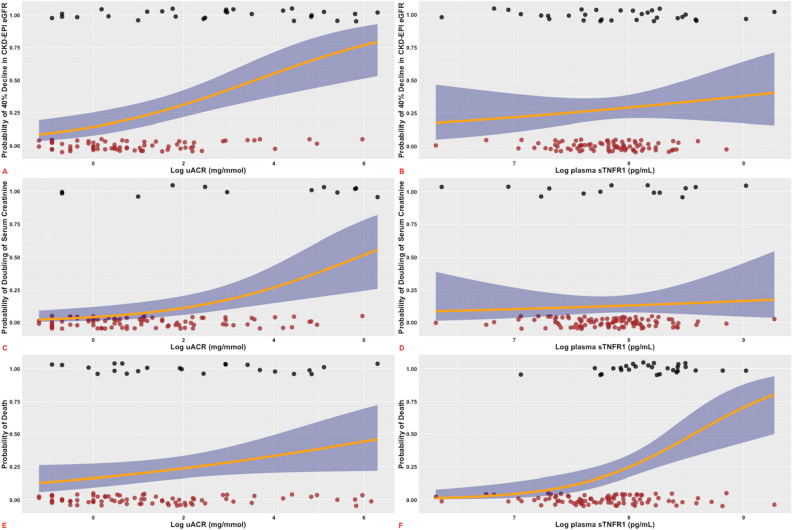
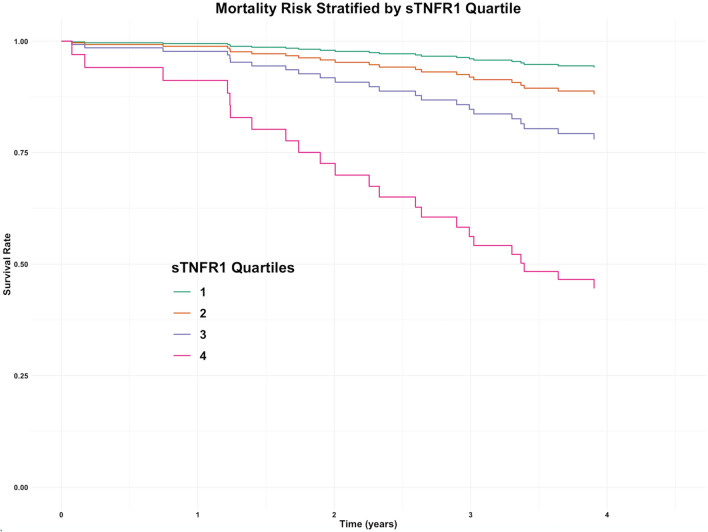
Identification of people with diabetes and chronic kidney disease at high-risk of early mortality is a priority to guide intensification of therapy. We aimed to investigate the complementary prognostic value of baseline urine albumin-to-creatinine ratio (uACR) and plasma soluble tumour necrosis factor receptor-1 (sTNFR1) with respect to early mortality and renal functional decline in a population with type 2 diabetes and advanced chronic kidney disease. We measured plasma sTNFR1 in people with type 2 diabetes (HbA ≥ 48 mmol/mol) at 2 hospital sites in Dublin between October 15th, 2014 and July 17th, 2015. In a subgroup of patients with advanced chronic kidney disease at baseline (estimated glomerular filtration rate (eGFR) ≤ 60 mL/min/BSA) (n = 118), we collected clinical and longitudinal laboratory data to investigate relationships between sTNFR1 and renal and mortality endpoints by multivariable linear mixed-effects models and Cox proportional hazards regression models. The cohort was 64% male and 97% Caucasian. Mean age was 74 years, with a median type 2 diabetes duration of 16 years. Mean CKD-EPI eGFR was 42 mL/min/BSA and median [IQR] uACR was 3 [11] mg/mmol. Twenty-three (39%) people in quartiles 3 and 4 for plasma sTNFR1 died over 4-year follow-up. After adjustment for clinical variables, annual CKD-EPI eGFR decreased by - 0.56 mL/min/BSA/year for each logarithm unit increase in baseline uACR, corresponding to an annual loss of renal function of 3% per year. Furthermore, elevated uACR, but not sTNFR1, increased the risk of ≥ 40% decline in CKD-EPI eGFR (HR 1.5, p = 0.001) and doubling of serum creatinine (HR 2.0, p < 0.001). Plasma sTNFR1 did not predict a more negative trajectory in eGFR slope. However, for those people in quartiles 3 and 4 for plasma sTNFR1, an increased risk of incident mortality was detected (HR 4.9, p = 0.02). No such association was detected for uACR. In this elderly cohort of patients with type 2 diabetes and chronic kidney disease, sTNFR1 predicted short-to-medium term mortality risk but not risk of progressive renal functional decline. In contrast, parallel assessment of uACR predicted renal functional decline but not mortality, highlighting the complementary prognostic information provided by both parameters.
识别患有糖尿病和慢性肾病且早期死亡率高的患者是指导强化治疗的重点。我们旨在研究基线尿白蛋白与肌酐比值(uACR)和血浆可溶性肿瘤坏死因子受体-1(sTNFR1)与 2 型糖尿病和晚期慢性肾病患者早期死亡率和肾功能下降的互补预后价值。我们于 2014 年 10 月 15 日至 2015 年 7 月 17 日在都柏林的 2 家医院测量了 2 型糖尿病患者(HbA ≥ 48mmol/mol)的血浆 sTNFR1。在基线时患有晚期慢性肾病的患者亚组(估计肾小球滤过率(eGFR)≤60mL/min/BSA)(n=118)中,我们收集了临床和纵向实验室数据,通过多变量线性混合效应模型和 Cox 比例风险回归模型研究 sTNFR1 与肾脏和死亡率终点之间的关系。该队列中 64%为男性,97%为白种人。平均年龄为 74 岁,中位 2 型糖尿病病程为 16 年。平均 CKD-EPI eGFR 为 42mL/min/BSA,中位数[IQR]uACR 为 3[11]mg/mmol。在 4 年随访期间,血浆 sTNFR1 在第 3 和第 4 四分位数的 23 人(39%)死亡。调整临床变量后,基线 uACR 每增加一个对数单位,每年 CKD-EPI eGFR 下降 -0.56mL/min/BSA/年,相当于每年肾功能下降 3%。此外,升高的 uACR 而非 sTNFR1 增加了 CKD-EPI eGFR 下降≥40%的风险(HR 1.5,p=0.001)和血清肌酐加倍的风险(HR 2.0,p<0.001)。血浆 sTNFR1 并未预测 eGFR 斜率的更负轨迹。然而,对于血浆 sTNFR1 在第 3 和第 4 四分位数的那些人,检测到发生死亡的风险增加(HR 4.9,p=0.02)。未发现 uACR 有这种关联。在这项患有 2 型糖尿病和慢性肾病的老年患者队列中,sTNFR1 预测了短期至中期死亡率风险,但不能预测肾功能进行性下降的风险。相比之下,平行评估 uACR 预测了肾功能下降,但不能预测死亡率,突出了这两个参数提供的互补预后信息。