Division of Gastroenterology, Hepatology, and Nutrition, University of Minnesota, Minneapolis, MN.
Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, MI.
Hepatology. 2021 Jun;73(6):2429-2440. doi: 10.1002/hep.31548. Epub 2021 Apr 19.
Patients with decompensated cirrhosis are prescribed numerous medications. Data are limited as to whether patients are receiving medications they need and avoiding those they do not. We examined a large national claims database (2010-2015) to characterize the complete medication profile as well as the factors associated with appropriate and potentially inappropriate medication use in 12,621 patients with decompensated cirrhosis.
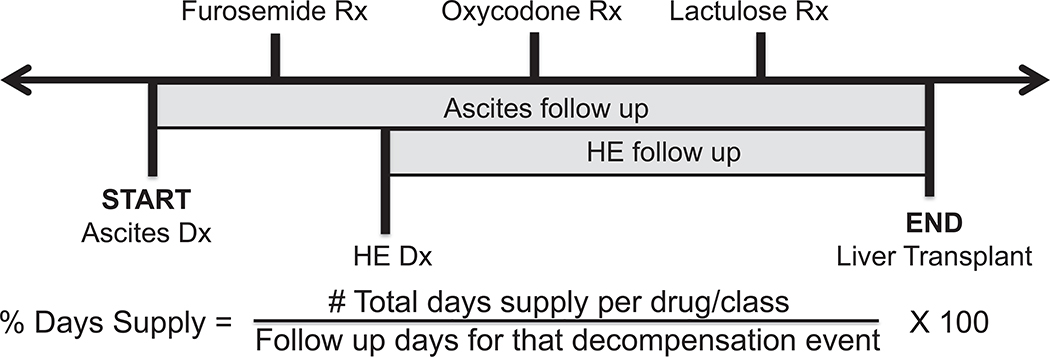
Clinical guidelines and existing literature were used to determine appropriate and potentially inappropriate medications in decompensated cirrhosis. The total medication days' supply was calculated from pharmacy data and divided by the follow-up period for each decompensation. Ascites was the most common (86.5%), followed by hepatic encephalopathy (HE; 37.8%), variceal bleeding (VB; 17.5%), hepatorenal syndrome (6.3%), and spontaneous bacterial peritonitis (SBP; 6.1%). For patients with ascites, 55.8% filled a diuretic. For patients with HE, 32.4% and 63.3% filled rifaximin and lactulose, respectively. After VB, 60.3% of patients filled a nonselective beta blocker, and after an episode of SBP, 48.0% of patients filled an antibiotic for prophylaxis. The minority (4.5%-17.3%) had enough medication to cover >50% follow-up days. Potentially inappropriate medication use was common: 53.2% filled an opiate, 46.0% proton pump inhibitors, 14.2% benzodiazepines, and 10.1% nonsteroidal anti-inflammatory drugs. Disease severity markers were associated with more appropriate mediation use but not consistently associated with less inappropriate medication use.
Patients with decompensated cirrhosis are not filling indicated medications as often or as long as is recommended and are also filling medications that are potentially harmful. Future steps include integrating pharmacy records with medical records to obtain a complete medication list and counseling on medication use with patients at each visit.
失代偿期肝硬化患者需要服用大量药物。目前对于失代偿期肝硬化患者是否正在服用所需药物以及避免服用非必需药物的数据有限。我们通过大型全国性理赔数据库(2010-2015 年),对 12621 例失代偿期肝硬化患者的完整药物使用情况以及与适当和潜在不适当药物使用相关的因素进行了研究。
我们使用临床指南和现有文献来确定失代偿期肝硬化中的适当和潜在不适当药物。根据药房数据计算药物总供应天数,并除以每次失代偿的随访时间。腹水是最常见的并发症(86.5%),其次是肝性脑病(HE;37.8%)、静脉曲张出血(VB;17.5%)、肝肾综合征(6.3%)和自发性细菌性腹膜炎(SBP;6.1%)。对于有腹水的患者,55.8%的患者服用利尿剂。对于有 HE 的患者,分别有 32.4%和 63.3%的患者服用利福昔明和乳果糖。VB 后,60.3%的患者服用非选择性β受体阻滞剂,SBP 后,48.0%的患者服用抗生素预防。少数患者(4.5%-17.3%)的药物足以覆盖超过 50%的随访天数。潜在不适当的药物使用很常见:53.2%的患者服用阿片类药物,46.0%的患者服用质子泵抑制剂,14.2%的患者服用苯二氮䓬类药物,10.1%的患者服用非甾体抗炎药。疾病严重程度标志物与更适当的药物治疗相关,但与更少的不适当药物治疗并不一致。
失代偿期肝硬化患者并未按照推荐的频率和时间服用所需药物,而且还在服用潜在有害的药物。未来的步骤包括将药房记录与病历整合,以获得完整的药物清单,并在每次就诊时为患者提供药物使用咨询。