Cheong Jeanie L Y, Olsen Joy E, Huang Li, Dalziel Kim M, Boland Rosemarie A, Burnett Alice C, Haikerwal Anjali, Spittle Alicia J, Opie Gillian, Stewart Alice E, Hickey Leah M, Anderson Peter J, Doyle Lex W
Clinical Sciences, Murdoch Children's Research Institute, Parkville, Victoria, Australia
Newborn Research, Royal Women's Hospital, Parkville, Victoria, Australia.
BMJ Open. 2020 Sep 10;10(9):e037507. doi: 10.1136/bmjopen-2020-037507.
It is unclear how newer methods of respiratory support for infants born extremely preterm (EP; 22-27 weeks gestation) have affected in-hospital sequelae. We aimed to determine changes in respiratory support, survival and morbidity in EP infants since the early 1990s.
Prospective longitudinal cohort study.
The State of Victoria, Australia.
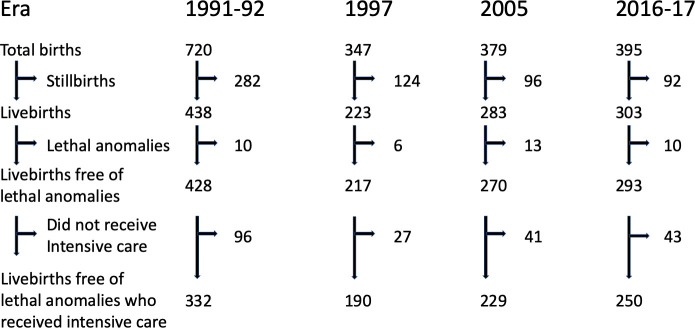
All EP births offered intensive care in four discrete eras (1991-1992 (24 months): n=332, 1997 (12 months): n=190, 2005 (12 months): n=229, and April 2016-March 2017 (12 months): n=250).
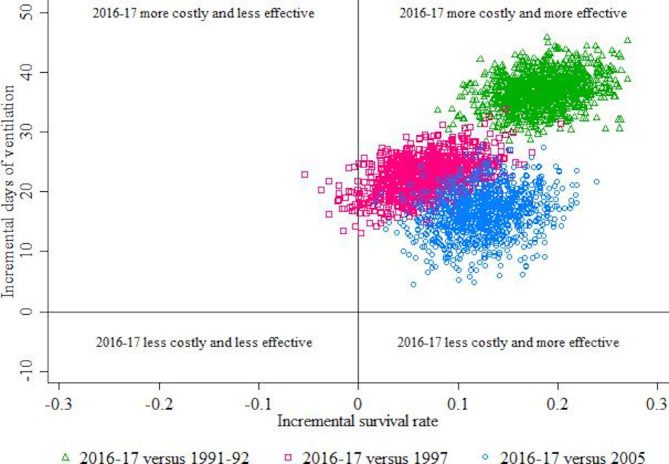
Consumption of respiratory support, survival and morbidity to discharge home. Cost-effectiveness ratios describing the average additional days of respiratory support associated per additional survivor were calculated.
Median duration of any respiratory support increased from 22 days (1991-1992) to 66 days (2016-2017). The increase occurred in non-invasive respiratory support (2 days (1991-1992) to 51 days (2016-2017)), with high-flow nasal cannulae, unavailable in earlier cohorts, comprising almost one-half of the duration in 2016-2017. Survival to discharge home increased (68% (1991-1992) to 87% (2016-2017)). Cystic periventricular leukomalacia decreased (6.3% (1991-1992) to 1.2% (2016-2017)), whereas retinopathy of prematurity requiring treatment increased (4.0% (1991-1992) to 10.0% (2016-2017)). The average additional costs associated with one additional infant surviving in 2016-2017 were 200 (95% CI 150 to 297) days, 326 (183 to 1127) days and 130 (70 to 267) days compared with 1991-1992, 1997 and 2005, respectively.
Consumption of resources for respiratory support has escalated with improved survival over time. Cystic periventricular leukomalacia reduced in incidence but retinopathy of prematurity requiring treatment increased. How these changes translate into long-term respiratory or neurological function remains to be determined.
目前尚不清楚针对极早产儿(孕周22 - 27周)的新型呼吸支持方法如何影响院内后遗症。我们旨在确定自20世纪90年代初以来极早产儿呼吸支持、生存及发病率的变化情况。
前瞻性纵向队列研究。
澳大利亚维多利亚州。
在四个不同时期(1991 - 1992年(24个月):n = 332,1997年(12个月):n = 190,2005年(12个月):n = 229,以及2016年4月 - 2017年3月(12个月):n = 250)接受重症监护的所有极早产儿。
呼吸支持的使用情况、生存情况及出院时的发病率。计算了描述每增加一名存活者所增加的呼吸支持平均天数的成本效益比。
任何呼吸支持的中位持续时间从1991 - 1992年的22天增加到2016 - 2017年的66天。这种增加发生在无创呼吸支持方面(从1991 - 1992年的2天增加到2016 - 2017年的51天),早期队列中没有的高流量鼻导管,在2016 - 2017年占持续时间的近一半。出院时的存活率有所提高(从1991 - 1992年的68%提高到2016 - 2017年的87%)。脑室周围白质软化症的发生率降低(从1991 - 1992年的6.3%降至2016 - 2017年的1.2%),而需要治疗的早产儿视网膜病变增加(从1991 - 1992年的4.0%升至2016 - 2017年的10.0%)。与1991 - 1992年、1997年和2005年相比,2016 - 2017年每多一名存活婴儿的平均额外成本分别为200(95%CI 150至297)天、326(183至1127)天和130(70至267)天。
随着时间的推移,随着存活率的提高,呼吸支持的资源消耗有所增加。脑室周围白质软化症的发病率降低,但需要治疗的早产儿视网膜病变增加。这些变化如何转化为长期呼吸或神经功能仍有待确定。