Koay Eugene J, Katz Matthew H G, Wang Huamin, Wang Xuemei, Prakash Laura, Javle Milind, Shroff Rachna, Fogelman David, Avila Santiago, Zaid Mohamed, Elganainy Dalia, Lee Yeonju, Crane Christopher H, Krishnan Sunil, Das Prajnan, Fleming Jason B, Lee Jeffrey E, Tamm Eric P, Bhosale Priya, Lee Jeffrey H, Weston Brian, Maitra Anirban, Wolff Robert A, Varadhachary Gauri R
University of Texas MD Anderson Cancer Center, Houston, TX.
Memorial Sloan Kettering Cancer Center, New York, NY.
JCO Precis Oncol. 2019 Aug 23;3. doi: 10.1200/PO.19.00001. eCollection 2019.
Effective preoperative regimens and biomarkers for pancreatic ductal adenocarcinoma (PDAC) are lacking. We prospectively evaluated fluorouracil, leucovorin, irinotecan, and oxaliplatin (FOLFIRINOX)-based treatment and imaging-based biomarkers for borderline resectable PDAC.
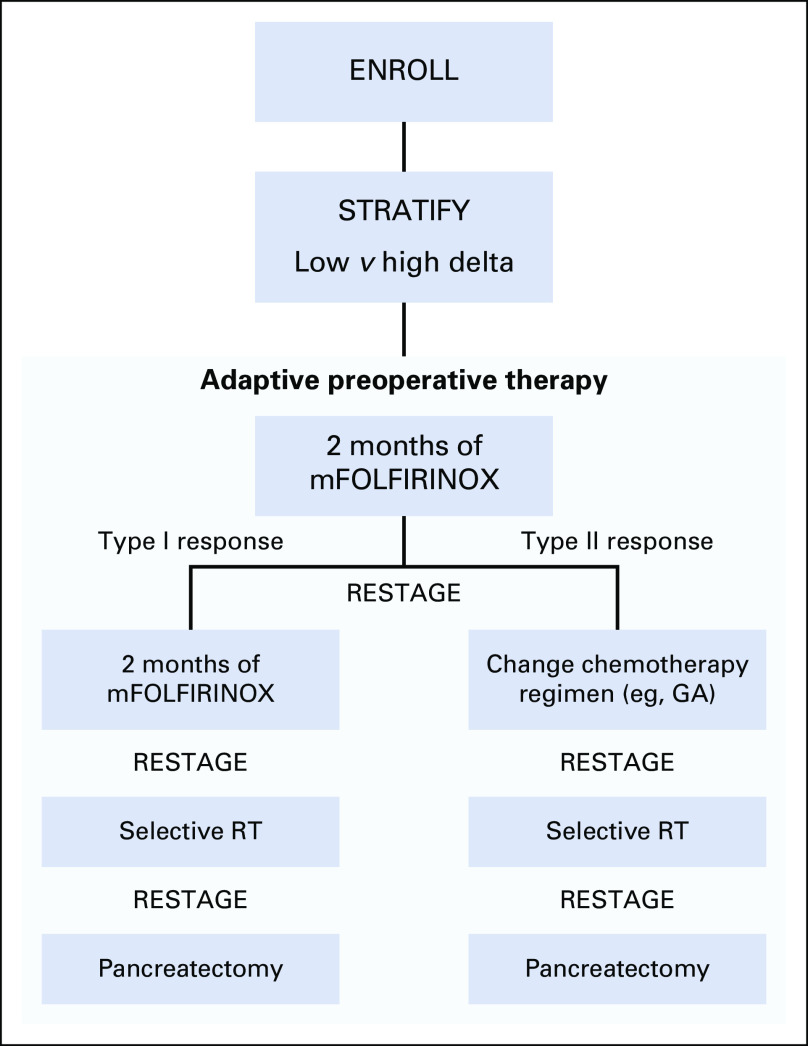
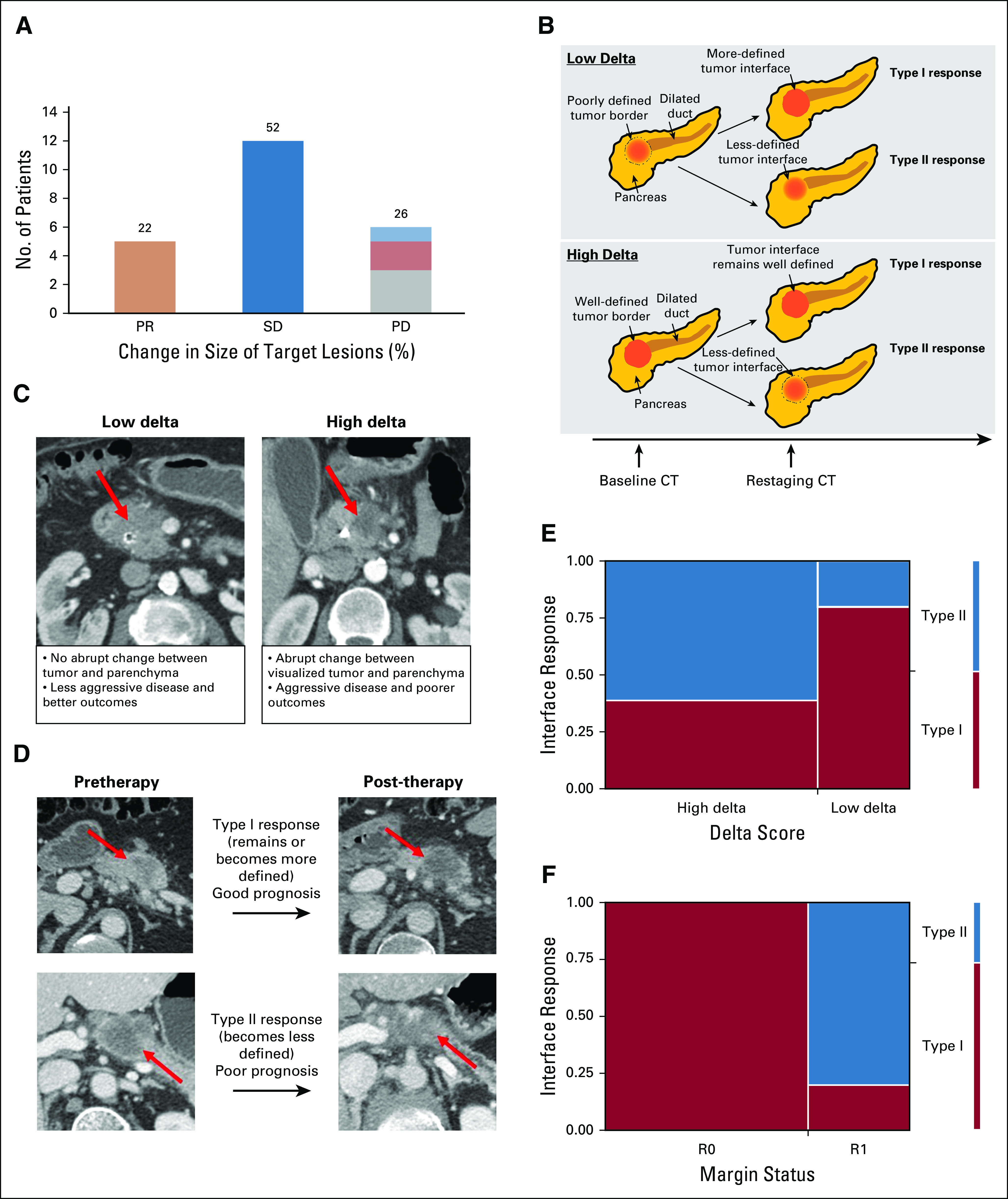
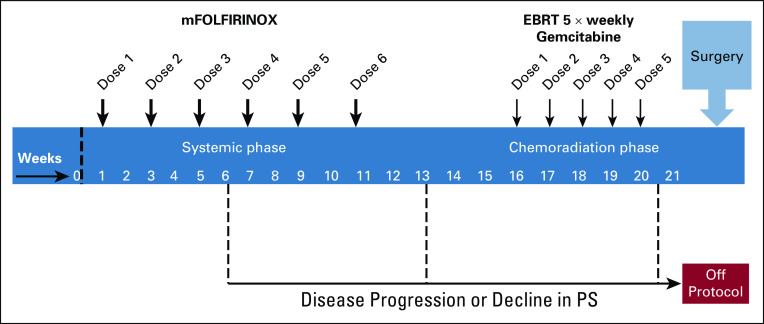
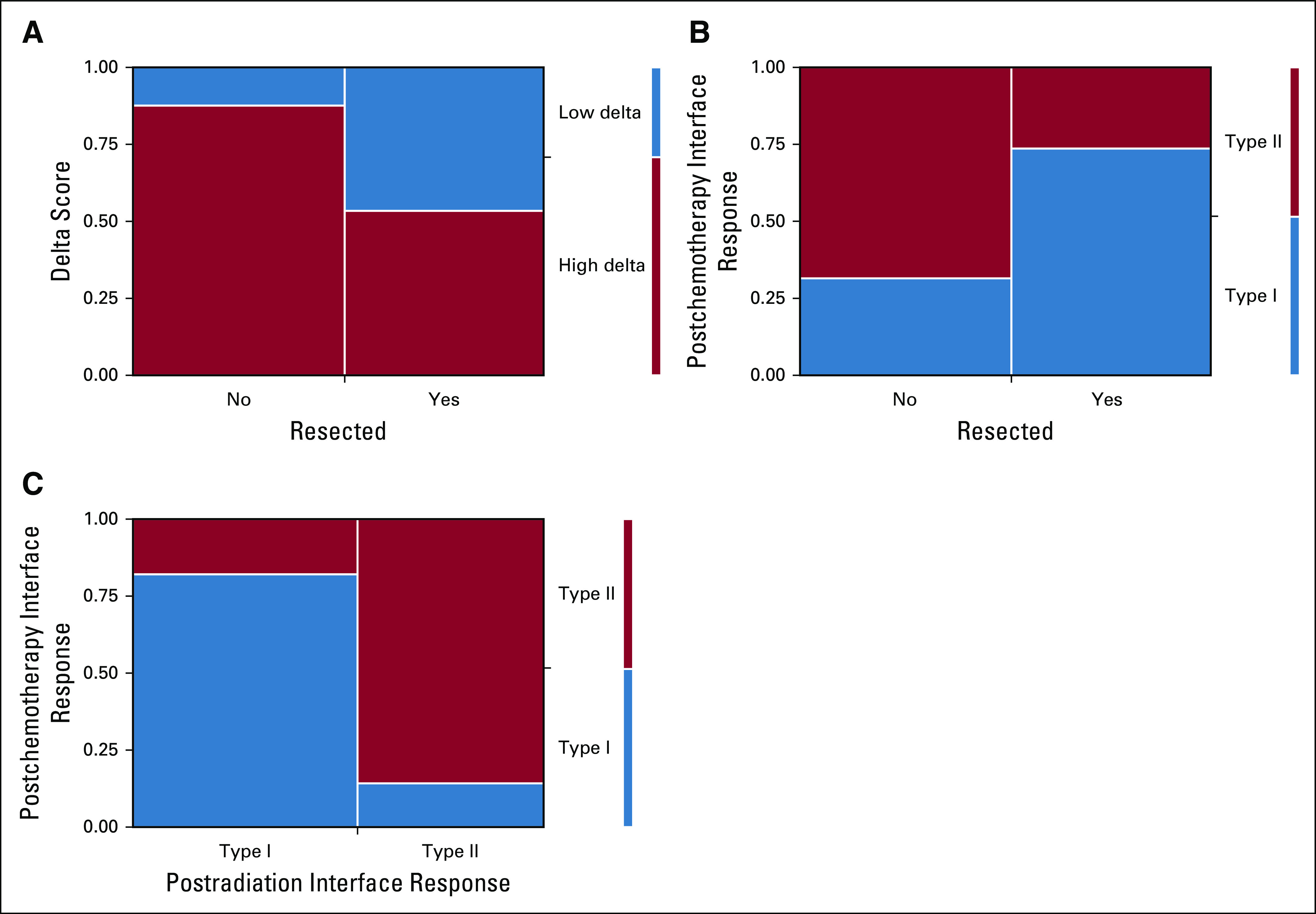
Eligible patients had treatment-naïve, histology-confirmed PDAC and one or more high-risk features: mesenteric vessel involvement, CA 19-9 level of 500 mg/dL or greater, and indeterminate metastatic lesions. Patients received modified FOLFIRINOX and chemoradiation before anticipated pancreatectomy. Tumors were classified on baseline computed tomography as high delta (well-defined interface with parenchyma) or low delta (ill-defined interface). We designated computed tomography interface response after therapy as type I (remained or became well defined) or type II (became ill defined). The study had 80% power to differentiate a 60% from 40% resection rate (α = .10). Overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier method, and subgroups were compared using log-rank tests.
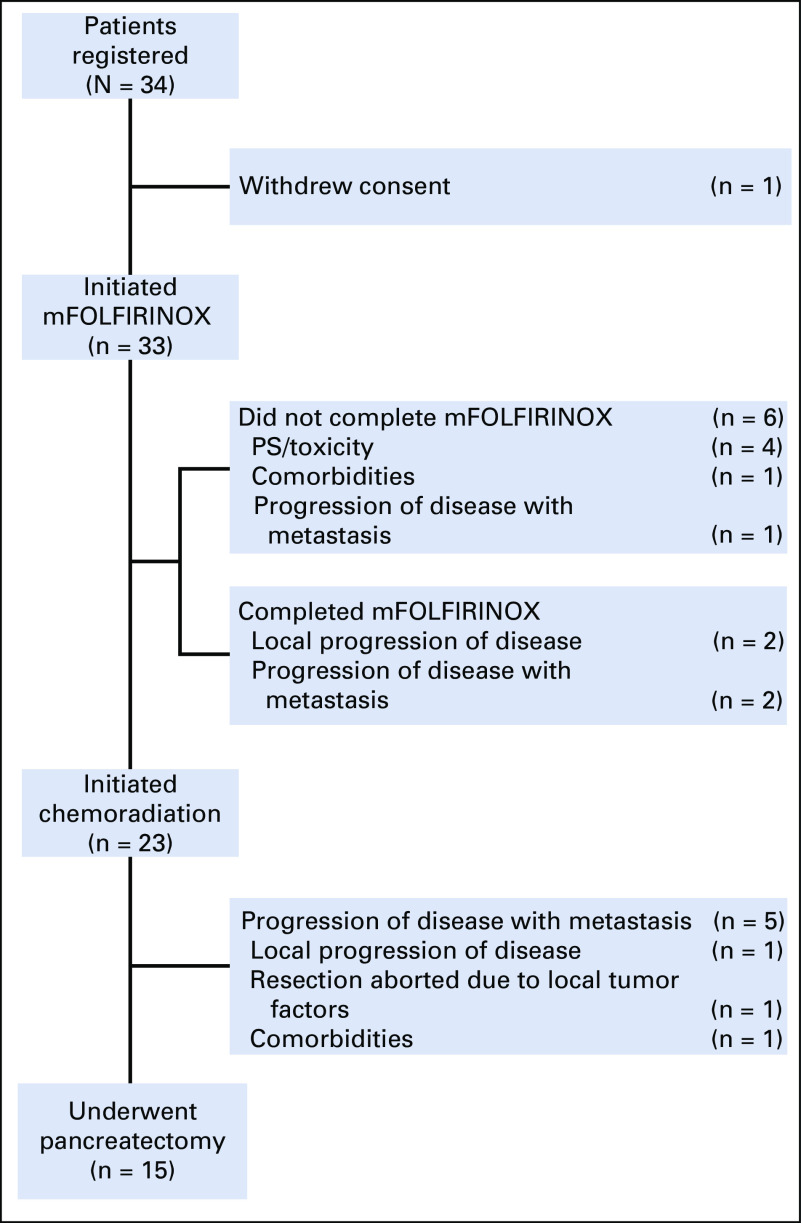
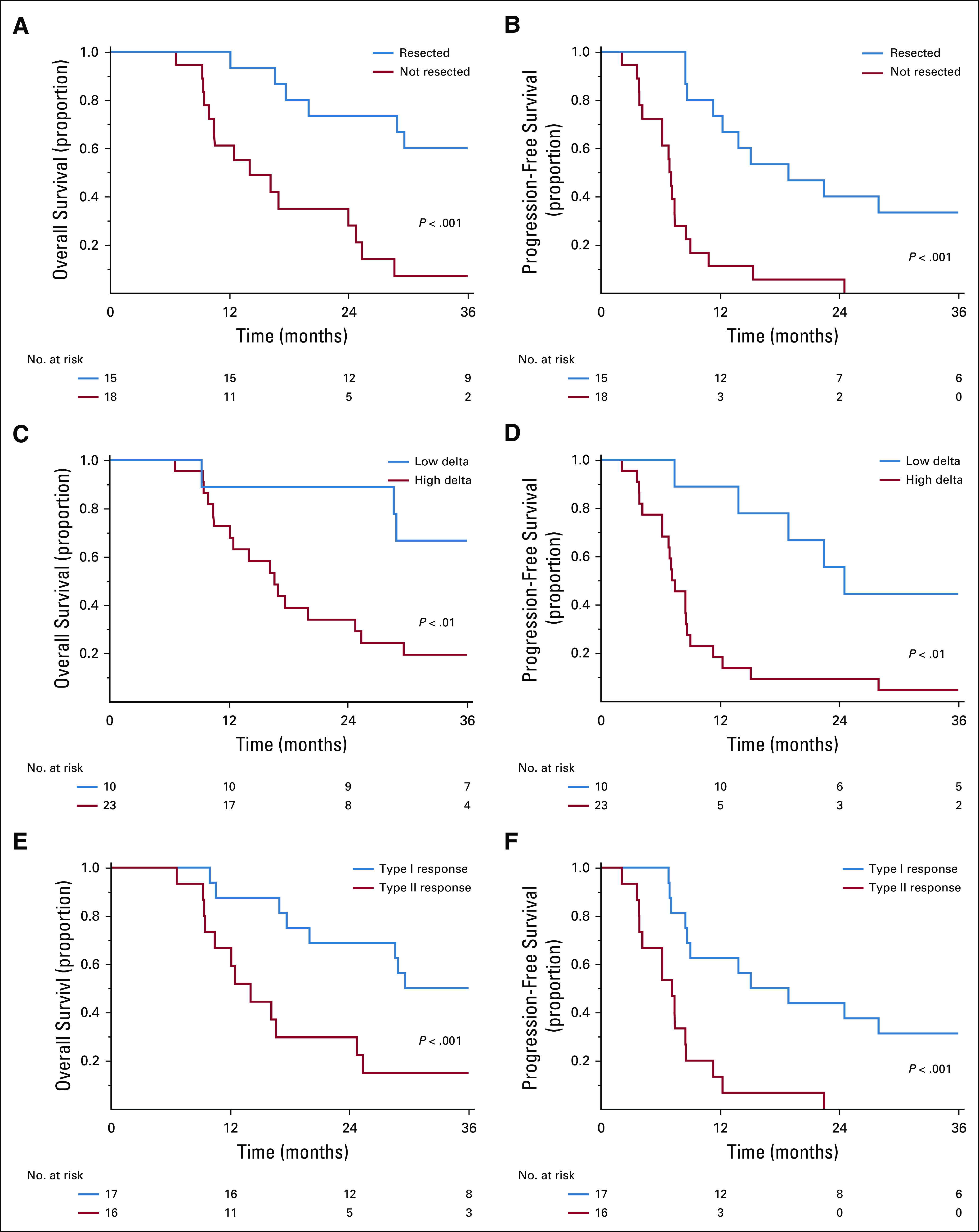
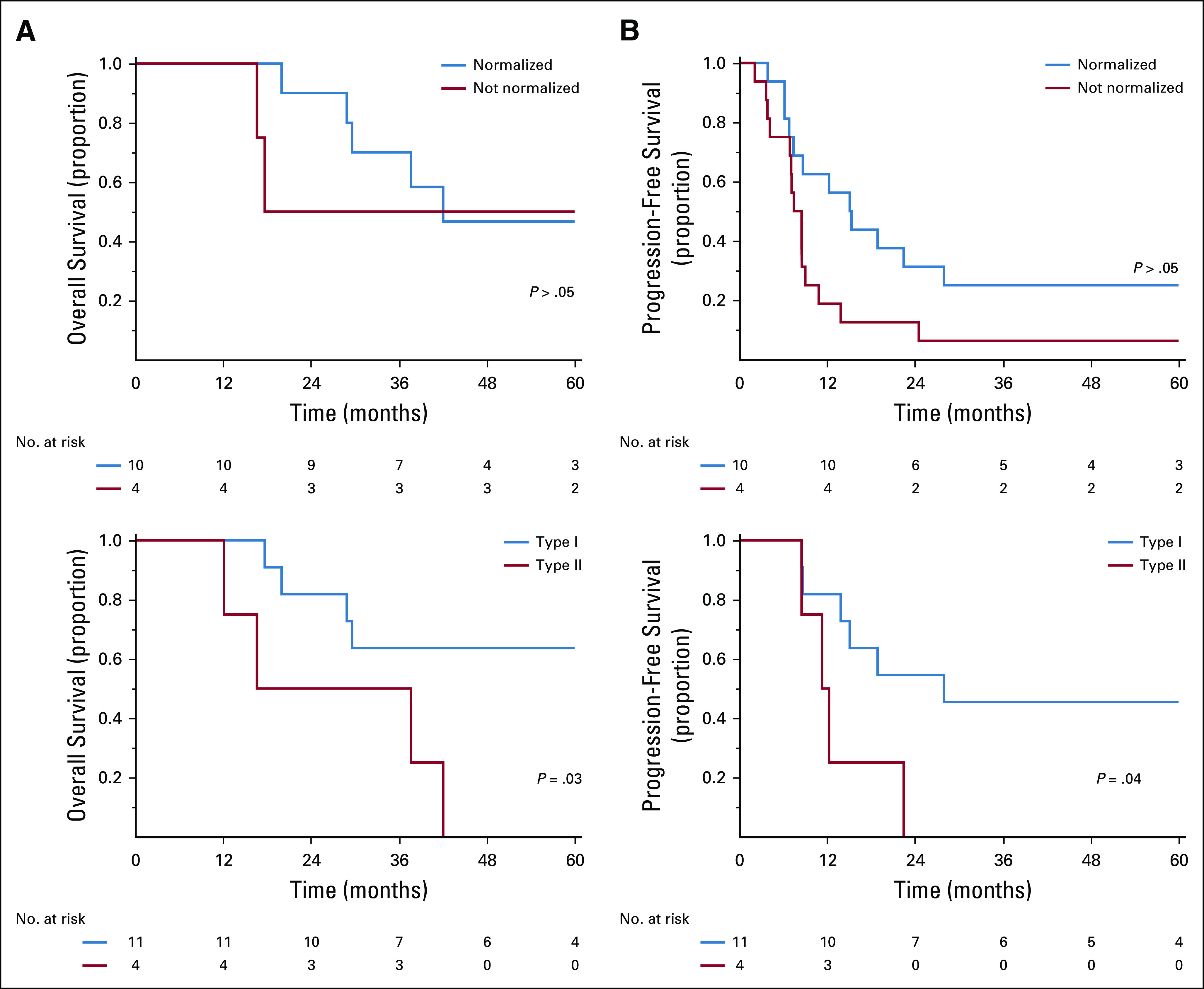
Thirty-three patients initiated therapy; 45% underwent pancreatectomy. The median OS was 24 months (95% CI, 16.2 to 29.6 months). For patients who did and did not undergo pancreatectomy, the median OS was 42 months (95% CI, 17.7 months to not estimable) and 14 months (95% CI, 9.0 to 24.8 months), respectively. Patients with high-delta tumors had lower 3-year PFS (4% 40%) and 3-year OS rates (20% 60%) than those with low-delta tumors (both < .05). Patients with type II interface responses had lower 3-year PFS (0% 29%) and 3-year OS rates (16% 47%) than those with type I responses (both < .001).
Preoperative FOLFIRINOX followed by chemoradiation for high-risk borderline resectable PDAC was associated with a resection rate of 45% and median OS of approximately 2 years. Our imaging-based biomarker validation indicates that personalized treatment may be achieved using these biomarkers at baseline and post-treatment.
目前缺乏针对胰腺导管腺癌(PDAC)的有效术前治疗方案和生物标志物。我们前瞻性地评估了基于氟尿嘧啶、亚叶酸钙、伊立替康和奥沙利铂(FOLFIRINOX)的治疗方案以及基于影像学的生物标志物在可切除边缘性PDAC中的应用。
符合条件的患者为未经治疗、组织学确诊的PDAC且具有一个或多个高危特征:肠系膜血管受累、CA 19-9水平≥500 mg/dL以及不确定的转移灶。患者在预期的胰腺切除术前接受改良的FOLFIRINOX和放化疗。根据基线计算机断层扫描将肿瘤分类为高δ(与实质界限清晰)或低δ(界限不清)。我们将治疗后的计算机断层扫描界面反应指定为I型(保持或变得界限清晰)或II型(变得界限不清)。该研究有80%的把握度区分60%和40%的切除率(α = 0.10)。采用Kaplan-Meier法估计总生存期(OS)和无进展生存期(PFS),并使用对数秩检验比较亚组。
33例患者开始治疗;45%接受了胰腺切除术。中位OS为24个月(95%CI,16.2至29.6个月)。接受和未接受胰腺切除术的患者,中位OS分别为42个月(95%CI,17.7个月至无法估计)和14个月(95%CI,9.0至24.8个月)。高δ肿瘤患者的3年PFS(4%对40%)和3年OS率(20%对60%)低于低δ肿瘤患者(均P < 0.05)。II型界面反应患者的3年PFS(0%对29%)和3年OS率(16%对47%)低于I型反应患者(均P < 0.001)。
对于高危可切除边缘性PDAC,术前采用FOLFIRINOX然后进行放化疗,切除率为45%,中位OS约为2年。我们基于影像学的生物标志物验证表明,使用这些基线和治疗后的生物标志物可能实现个性化治疗。