From the Department of Anesthesiology, Section on Critical Care Medicine, Wake Forest School of Medicine, Winston-Salem, North Carolina.
Outcomes Research Consortium, Cleveland, Ohio.
Anesth Analg. 2020 Oct;131(4):1012-1024. doi: 10.1213/ANE.0000000000004788.
Opioid-related adverse events are a serious problem in hospitalized patients. Little is known about patients who are likely to experience opioid-induced respiratory depression events on the general care floor and may benefit from improved monitoring and early intervention. The trial objective was to derive and validate a risk prediction tool for respiratory depression in patients receiving opioids, as detected by continuous pulse oximetry and capnography monitoring.
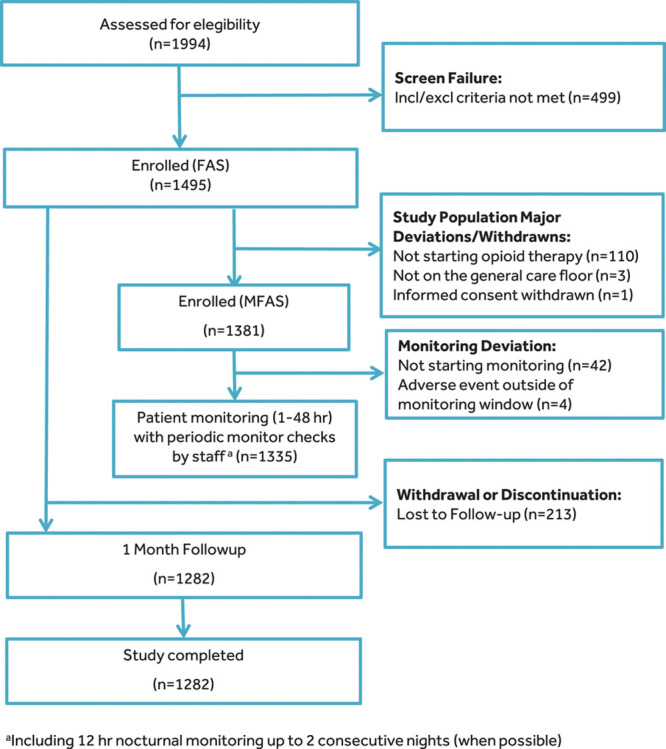
PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY) was a prospective, observational trial of blinded continuous capnography and oximetry conducted at 16 sites in the United States, Europe, and Asia. Vital signs were intermittently monitored per standard of care. A total of 1335 patients receiving parenteral opioids and continuously monitored on the general care floor were included in the analysis. A respiratory depression episode was defined as respiratory rate ≤5 breaths/min (bpm), oxygen saturation ≤85%, or end-tidal carbon dioxide ≤15 or ≥60 mm Hg for ≥3 minutes; apnea episode lasting >30 seconds; or any respiratory opioid-related adverse event. A risk prediction tool was derived using a multivariable logistic regression model of 46 a priori defined risk factors with stepwise selection and was internally validated by bootstrapping.
One or more respiratory depression episodes were detected in 614 (46%) of 1335 general care floor patients (43% male; mean age, 58 ± 14 years) continuously monitored for a median of 24 hours (interquartile range [IQR], 17-26). A multivariable respiratory depression prediction model with area under the curve of 0.740 was developed using 5 independent variables: age ≥60 (in decades), sex, opioid naivety, sleep disorders, and chronic heart failure. The PRODIGY risk prediction tool showed significant separation between patients with and without respiratory depression (P < .001) and an odds ratio of 6.07 (95% confidence interval [CI], 4.44-8.30; P < .001) between the high- and low-risk groups. Compared to patients without respiratory depression episodes, mean hospital length of stay was 3 days longer in patients with ≥1 respiratory depression episode (10.5 ± 10.8 vs 7.7 ± 7.8 days; P < .0001) identified using continuous oximetry and capnography monitoring.
A PRODIGY risk prediction model, derived from continuous oximetry and capnography, accurately predicts respiratory depression episodes in patients receiving opioids on the general care floor. Implementation of the PRODIGY score to determine the need for continuous monitoring may be a first step to reduce the incidence and consequences of respiratory compromise in patients receiving opioids on the general care floor.
阿片类药物相关的不良事件是住院患者的一个严重问题。对于可能在普通护理病房经历阿片类药物引起的呼吸抑制事件并可能受益于改善监测和早期干预的患者,知之甚少。该试验的目的是开发和验证一种用于检测接受阿片类药物治疗的患者呼吸抑制的风险预测工具,该工具通过连续脉搏血氧仪和呼气末二氧化碳监测进行检测。
接受连续脉搏血氧仪和呼气末二氧化碳监测的阿片类药物诱导性呼吸抑制预测(PRODIGY)是一项在美国、欧洲和亚洲 16 个地点进行的前瞻性、观察性、连续呼气末二氧化碳和血氧饱和度监测的盲法试验。根据标准护理间歇性监测生命体征。共纳入 1335 名在普通护理病房接受肠外阿片类药物治疗并持续监测的患者进行分析。呼吸抑制发作定义为呼吸频率≤5 次/分钟(bpm),氧饱和度≤85%,或呼气末二氧化碳≤15 或≥60mmHg 持续≥3 分钟;呼吸暂停发作持续时间>30 秒;或任何与呼吸相关的阿片类药物不良事件。使用 46 个预先定义的风险因素的多变量逻辑回归模型,通过逐步选择来推导风险预测工具,并通过自举法进行内部验证。
在 1335 名接受连续监测的普通护理病房患者中(43%为男性;平均年龄 58±14 岁),有 1 名或 1 名以上呼吸抑制发作的患者为 614 名(46%),中位监测时间为 24 小时(四分位距[IQR],17-26)。使用 5 个独立变量开发了一个具有 0.740 曲线下面积的多变量呼吸抑制预测模型:年龄≥60 岁(以十年为单位)、性别、阿片类药物初治、睡眠障碍和慢性心力衰竭。PRODIGY 风险预测工具在有和无呼吸抑制的患者之间有显著的区分(P<.001),高危组和低危组之间的比值比为 6.07(95%置信区间[CI],4.44-8.30;P<.001)。与无呼吸抑制发作的患者相比,有≥1 次呼吸抑制发作的患者的平均住院时间延长了 3 天(10.5±10.8 天比 7.7±7.8 天;P<.0001),使用连续血氧仪和呼气末二氧化碳监测可以发现这些患者。
从连续血氧仪和呼气末二氧化碳监测中得出的 PRODIGY 风险预测模型,可准确预测接受普通护理病房阿片类药物治疗的患者的呼吸抑制发作。实施 PRODIGY 评分来确定是否需要连续监测,可能是减少普通护理病房接受阿片类药物治疗的患者呼吸受损发生率和后果的第一步。