Wake Forest School of Medicine, Winston-Salem, NC, USA.
Outcomes Research Consortium, Cleveland, OH, USA.
BMC Anesthesiol. 2021 Mar 20;21(1):88. doi: 10.1186/s12871-021-01307-8.
Opioid-induced respiratory depression is common on the general care floor. However, the clinical and economic burden of respiratory depression is not well-described. The PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY) trial created a prediction tool to identify patients at risk of respiratory depression. The purpose of this retrospective sub-analysis was to examine healthcare utilization and hospital cost associated with respiratory depression.
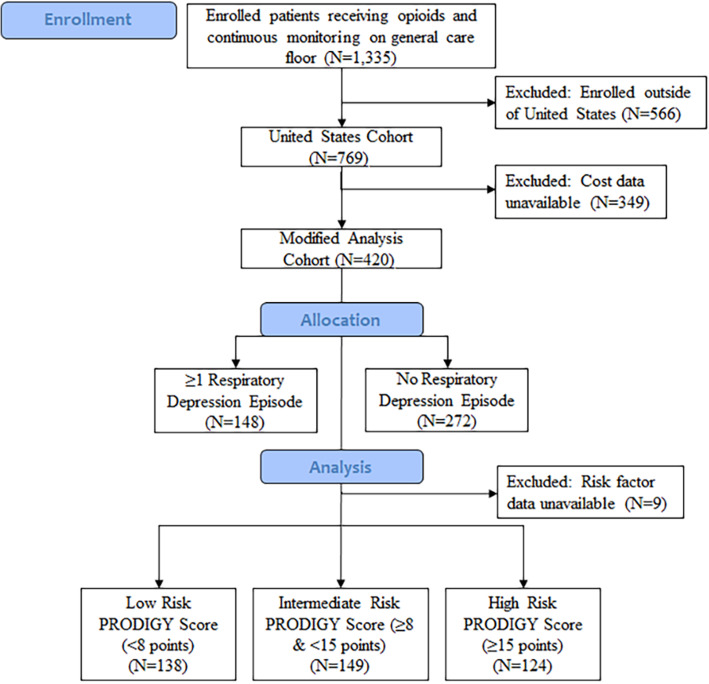
One thousand three hundred thirty-five patients (N = 769 United States patients) enrolled in the PRODIGY trial received parenteral opioids and underwent continuous capnography and pulse oximetry monitoring. Cost data was retrospectively collected for 420 United States patients. Differences in healthcare utilization and costs between patients with and without ≥1 respiratory depression episode were determined. The impact of respiratory depression on hospital cost per patient was evaluated using a propensity weighted generalized linear model.
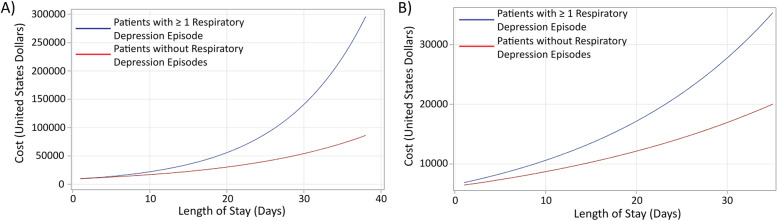
Patients with ≥1 respiratory depression episode had a longer length of stay (6.4 ± 7.8 days vs 5.0 ± 4.3 days, p = 0.009) and higher hospital cost ($21,892 ± $11,540 vs $18,206 ± $10,864, p = 0.002) compared to patients without respiratory depression. Patients at high risk for respiratory depression, determined using the PRODIGY risk prediction tool, who had ≥1 respiratory depression episode had higher hospital costs compared to high risk patients without respiratory depression ($21,948 ± $9128 vs $18,474 ± $9767, p = 0.0495). Propensity weighted analysis identified 17% higher costs for patients with ≥1 respiratory depression episode (p = 0.007). Length of stay significantly increased total cost, with cost increasing exponentially for patients with ≥1 respiratory depression episode as length of stay increased.
Respiratory depression on the general care floor is associated with a significantly longer length of stay and increased hospital costs. Early identification of patients at risk for respiratory depression, along with early proactive intervention, may reduce the incidence of respiratory depression and its associated clinical and economic burden.
ClinicalTrials.gov , NCT02811302 .
阿片类药物引起的呼吸抑制在普通病房很常见。然而,呼吸抑制的临床和经济负担并没有得到很好的描述。预测阿片类药物诱导的呼吸抑制患者监测 capnoGraphY (PRODIGY) 试验创建了一个预测工具,以确定有呼吸抑制风险的患者。本回顾性亚分析的目的是研究与呼吸抑制相关的医疗保健利用和医院成本。
1335 名(N=769 名美国患者)接受 PRODIGY 试验的患者接受了肠外阿片类药物治疗,并接受了连续的 capnography 和脉搏血氧饱和度监测。回顾性收集了 420 名美国患者的成本数据。确定了有≥1 次呼吸抑制发作与无呼吸抑制发作患者之间的医疗保健利用和成本差异。使用倾向加权广义线性模型评估呼吸抑制对每位患者住院费用的影响。
有≥1 次呼吸抑制发作的患者住院时间更长(6.4±7.8 天 vs 5.0±4.3 天,p=0.009),住院费用更高(21892±11540 美元 vs 18206±10864 美元,p=0.002)与无呼吸抑制的患者相比。使用 PRODIGY 风险预测工具确定有呼吸抑制高风险的患者,如果有≥1 次呼吸抑制发作,其住院费用高于无呼吸抑制的高风险患者(21948±9128 美元 vs 18474±9767 美元,p=0.0495)。倾向加权分析发现,有≥1 次呼吸抑制发作的患者成本增加了 17%(p=0.007)。住院时间显著增加了总费用,随着呼吸抑制发作次数的增加,住院时间的增加使成本呈指数级增加。
普通病房的呼吸抑制与住院时间明显延长和住院费用增加有关。早期识别有呼吸抑制风险的患者,并及早采取积极的干预措施,可能会降低呼吸抑制的发生率及其相关的临床和经济负担。
ClinicalTrials.gov,NCT02811302。