From the Department of Anesthesia & Perioperative Care, University of California, San Francisco, San Francisco, California.
Center for Gerontology and Department of Statistics, Virginia Tech, Blacksburg, VA.
Anesth Analg. 2020 Oct;131(4):1228-1236. doi: 10.1213/ANE.0000000000004713.
Recent limited evidence suggests that the use of a processed electroencephalographic (EEG) monitor to guide anesthetic management may influence postoperative cognitive outcomes; however, the mechanism is unclear.
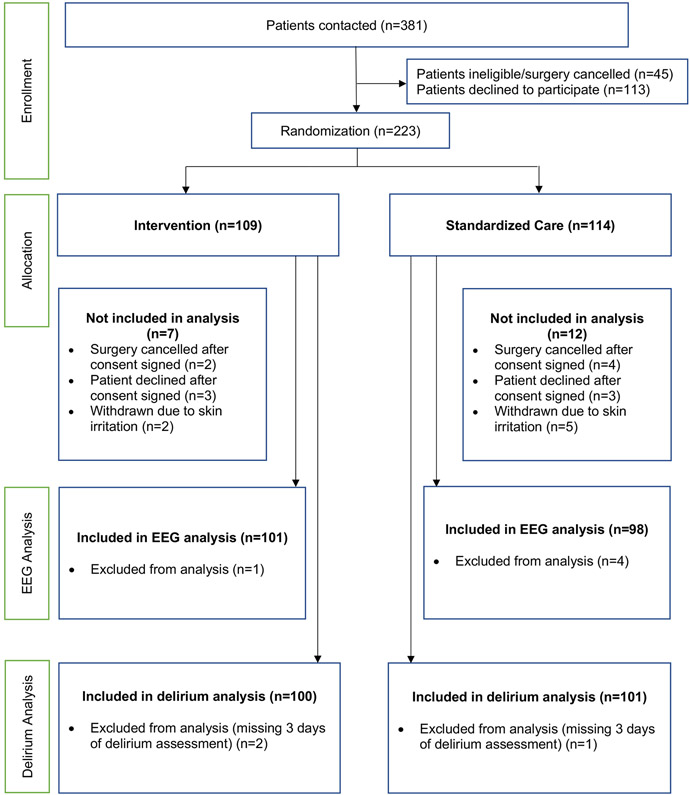
This exploratory, single-center, randomized clinical trial included patients who were ≥65 years of age undergoing elective noncardiac surgery. The study aimed to determine whether monitoring the brain using a processed EEG monitor reduced EEG suppression and subsequent postoperative delirium. The interventional group received processed EEG-guided anesthetic management to keep the Patient State Index (PSI) above 35 computed by the SEDline Brain Function Monitor (Masimo, Inc, Irvine, CA), while the standard care group was also monitored, but the EEG data were blinded from the clinicians. The primary outcome was intraoperative EEG suppression. A secondary outcome was incident postoperative delirium during the first 3 days after surgery.
All outcomes were analyzed using the intention-to-treat paradigm. Two hundred and four patients with a mean age of 72 ± 5 years were studied. Minutes of EEG suppression adjusted by the length of surgery was found to be less for the interventional group than the standard care group (median [interquartile range], 1.4% [5.0%] and 2.5% [10.4%]; Hodges-Lehmann estimated median difference [95% confidence interval {CI}] of -0.8% [-2.1 to -0.000009]). The effect of the intervention on EEG suppression differed for those with and without preoperative cognitive impairment (interaction P = .01), with the estimated incidence rate ratio (95% CI) of 0.39 (0.33-0.44) for those with preoperative cognitive impairment and 0.48 (0.44-0.51) for those without preoperative cognitive impairment. The incidence of delirium was not found to be different between the interventional (17%) and the standard care groups (20%), risk ratio = 0.85 (95% CI, 0.47-1.5).
The use of processed EEG to maintain the PSI >35 was associated with less time spent in intraoperative EEG suppression. Preoperative cognitive impairment was associated with a greater percent of surgical time spent in EEG suppression. A larger prospective cohort study to include more cognitively vulnerable patients is necessary to show whether an intervention to reduce EEG suppression is efficacious in reducing postoperative delirium.
最近有限的证据表明,使用经处理的脑电图(EEG)监测仪来指导麻醉管理可能会影响术后认知结果;然而,其机制尚不清楚。
这是一项探索性、单中心、随机临床试验,纳入了年龄≥65 岁接受择期非心脏手术的患者。该研究旨在确定使用经处理的脑电图监测仪监测大脑是否可以减少脑电图抑制和随后的术后谵妄。干预组接受经处理的脑电图引导的麻醉管理,以保持 SEDline 脑功能监测仪(Masimo,Inc,Irvine,CA)计算的患者状态指数(PSI)高于 35,而标准护理组也接受监测,但脑电图数据对临床医生是盲态的。主要结局是术中脑电图抑制。次要结局是术后 3 天内发生术后谵妄。
所有结局均采用意向治疗分析。204 名平均年龄 72±5 岁的患者接受了研究。与标准护理组相比,干预组术中脑电图抑制的时间更短(经手术时间校正,中位数[四分位数间距],1.4%[5.0%]和 2.5%[10.4%];Hodges-Lehmann 估计中位数差值[95%置信区间{CI}]为-0.8%[-2.1 至-0.000009])。该干预措施对脑电图抑制的影响因术前认知障碍的有无而不同(交互 P=.01),术前认知障碍患者的估计发病率比(95%CI)为 0.39(0.33-0.44),无术前认知障碍患者为 0.48(0.44-0.51)。干预组(17%)和标准护理组(20%)的谵妄发生率无差异,风险比=0.85(95%CI,0.47-1.5)。
使用经处理的脑电图将 PSI>35 与术中脑电图抑制时间减少相关。术前认知障碍与更多的手术时间脑电图抑制相关。需要进行更大的前瞻性队列研究,纳入更多认知脆弱的患者,以确定减少脑电图抑制的干预措施是否能有效减少术后谵妄。