Soehle Martin, Dittmann Alexander, Ellerkmann Richard K, Baumgarten Georg, Putensen Christian, Guenther Ulf
Department of Anaesthesiology and Intensive Care Medicine, University of Bonn, Bonn, Germany.
Department of Neurology and Psychiatry, LVR-Clinic, Bonn, Germany.
BMC Anesthesiol. 2015 Apr 28;15:61. doi: 10.1186/s12871-015-0051-7.
Postoperative delirium (POD) occurs frequently after cardiac surgery and is associated with increased morbidity and mortality. We analysed whether perioperative bilateral BIS monitoring may detect abnormalities before the onset of POD in cardiac surgery patients.
In a prospective observational study, 81 patients undergoing cardiac surgery were included. Bilateral Bispectral Index (BIS)-monitoring was applied during the pre-, intra- and postoperative period, and BIS, EEG Asymmetry (ASYM), and Burst Suppression Ratio (BSR) were recorded. POD was diagnosed according to the Confusion Assessment Method for the Intensive Care Unit, and patients were divided into a delirium and non-delirium group.
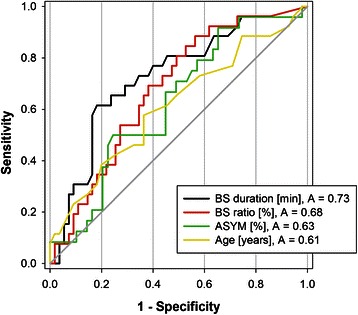
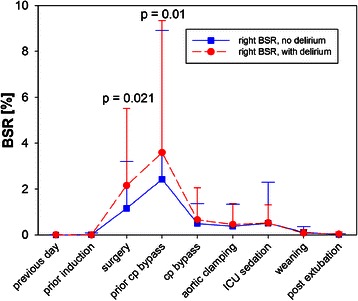
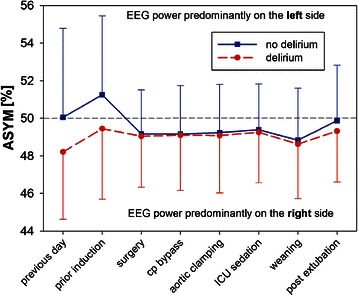
POD was detected in 26 patients (32%). A trend towards a lower ASYM was observed in the delirium group as compared to the non-delirium group on the preoperative day (ASYM = 48.2 ± 3.6% versus 50.0 ± 4.7%, mean ± sd, p = 0.087) as well as before induction of anaesthesia, with oral midazolam anxiolysis (median ASYM = 49.5%, IQR [47.4;51.5] versus 50.6%, IQR [49.1;54.2], p = 0.081). Delirious patients remained significantly (p = 0.018) longer in a burst suppression state intraoperatively (107 minutes, IQR [47;170] versus 44 minutes, IQR [11;120]) than non-delirious patients. Receiver operating analysis revealed burst suppression duration (area under the curve = 0.73, p = 0.001) and BSR (AUC = 0.68, p = 0.009) as predictors of POD.
Intraoperative assessment of BSR may identify patients at risk of POD and should be investigated in further studies. So far it remains unknown whether there is a causal relationship or rather an association between intraoperative burst suppression and the development of POD.
clinicaltrials.gov NCT01048775.
心脏手术后经常发生术后谵妄(POD),且与发病率和死亡率增加相关。我们分析了围手术期双侧脑电双频指数(BIS)监测是否能在心脏手术患者发生POD之前检测到异常。
在一项前瞻性观察研究中,纳入了81例行心脏手术的患者。在术前、术中和术后均应用双侧脑电双频指数(BIS)监测,并记录BIS、脑电图不对称性(ASYM)和爆发抑制率(BSR)。根据重症监护病房的谵妄评估方法诊断POD,并将患者分为谵妄组和非谵妄组。
26例患者(32%)检测到POD。与非谵妄组相比,谵妄组在术前一天(ASYM = 48.2±3.6% 对 50.0±4.7%,均值±标准差,p = 0.087)以及在使用口服咪达唑仑进行麻醉前焦虑缓解时,观察到ASYM有降低趋势(ASYM中位数 = 49.5%,四分位数间距[47.4;51.5] 对 50.6%,四分位数间距[49.1;54.2],p = 0.081)。谵妄患者术中处于爆发抑制状态的时间(107分钟,四分位数间距[47;170])比非谵妄患者(44分钟,四分位数间距[11;120])显著更长(p = 0.018)。受试者工作分析显示爆发抑制持续时间(曲线下面积 = 0.73,p = 0.001)和BSR(AUC = 0.68,p = 0.009)是POD的预测指标。
术中对BSR的评估可能识别出有POD风险的患者,应在进一步研究中进行调查。到目前为止,术中爆发抑制与POD的发生之间是因果关系还是仅仅是一种关联尚不清楚。
clinicaltrials.gov NCT01048775。