Virology Unit, Institut Pasteur du Cambodge, Institut Pasteur International Network, Phnom Penh, Cambodia.
Laboratoire de mathématiques d'Orsay, Université Paris-Saclay, CNRS, Inria, Orsay, France.
PLoS Negl Trop Dis. 2020 Sep 14;14(9):e0008603. doi: 10.1371/journal.pntd.0008603. eCollection 2020 Sep.
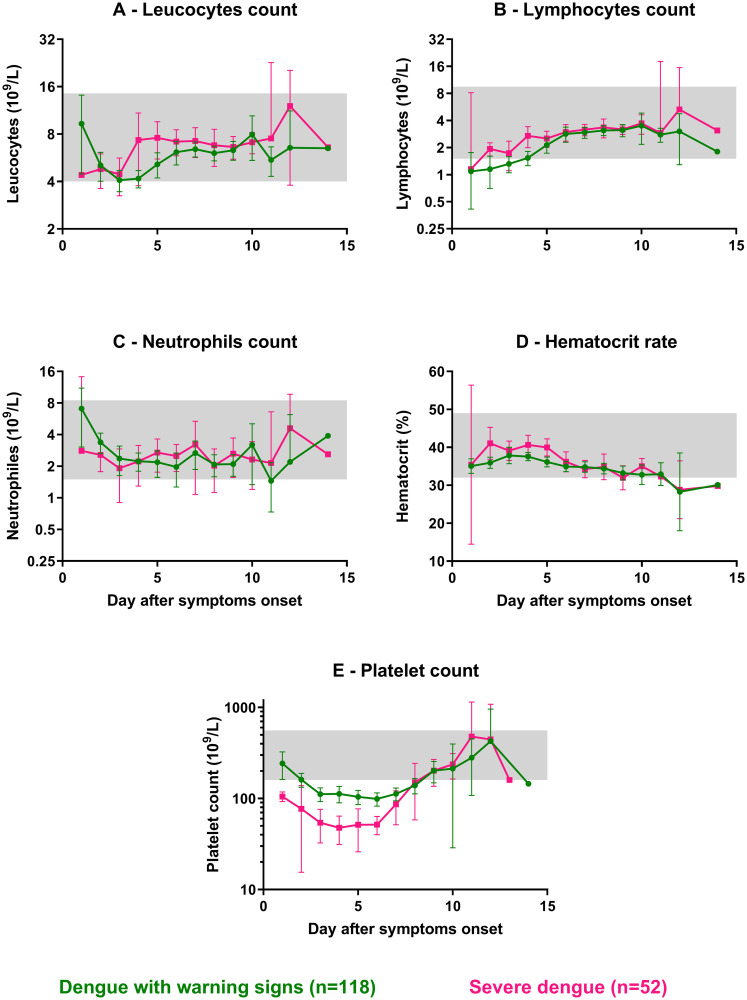
The World Health Organization (WHO) proposed guidelines on dengue clinical classification in 1997 and more recently in 2009 for the clinical management of patients. The WHO 1997 classification defines three categories of dengue infection according to severity: dengue fever (DF), dengue hemorrhagic fever (DHF), and dengue shock syndrome (DSS). Alternative WHO 2009 guidelines provide a cross-sectional classification aiming to discriminate dengue fever from dengue with warning signs (DWWS) and severe dengue (SD). The primary objective of this study was to perform a comparison of two dengue classifications. The secondary objective was to describe the changes of hematological and biochemical parameters occurring in patients presenting with different degrees of severity during the course of the disease, since progression to more severe clinical forms is unpredictable.
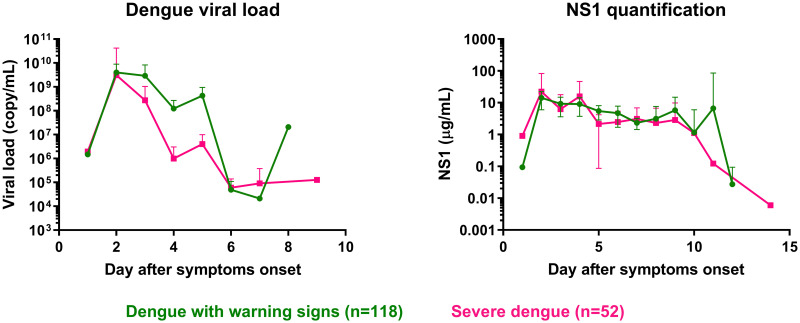
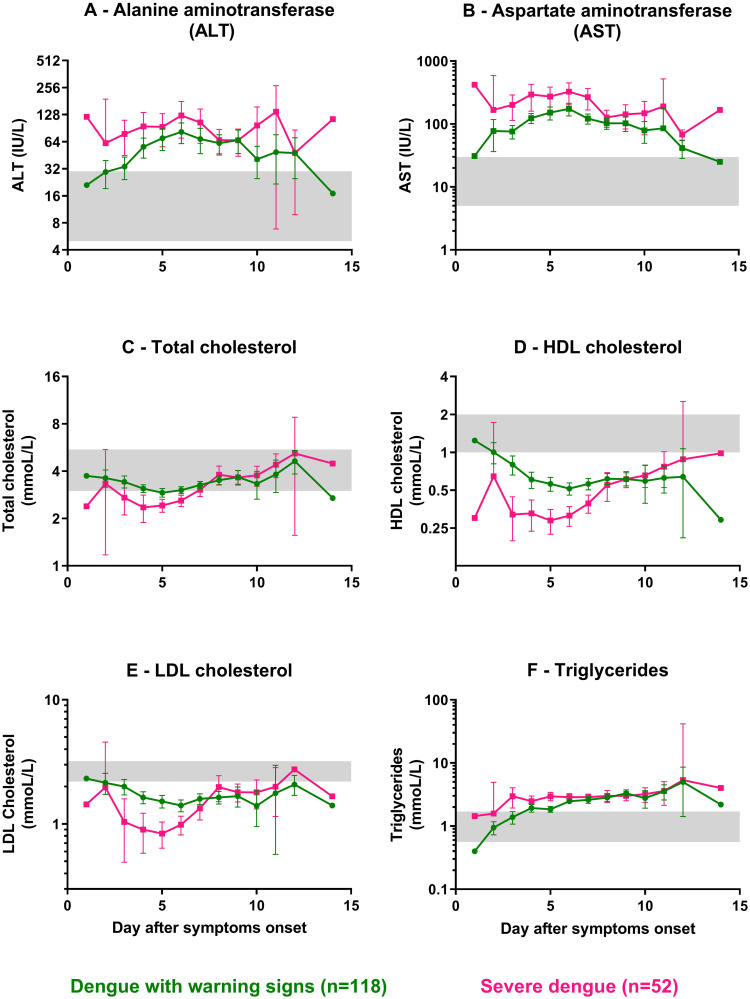
METHODOLOGY/PRINCIPAL FINDINGS: We performed a prospective, monocentric, cross-sectional study of hospitalized children in Cambodia, aged from 2 to 15 years old with severe and non-severe dengue. We enrolled 243 patients with acute dengue-like illness: 71.2% were dengue infections confirmed using quantitative reverse transcription PCR or NS1 antigen capture ELISA, of which 87.2% and 9.0% of DF cases were respectively classified DWWS and SD, and 35.9% of DHF were designated SD using an adapted WHO 2009 classification for SD case definition. Systematic use of ultrasound at patient admission was crucial for detecting plasma leakage. No difference was observed in the concentration of secreted NS1 protein between different dengue severity groups. Lipid profiles were different between DWWS and SD at admission, characterized by a decrease in total cholesterol, HDL cholesterol, and LDL cholesterol, in SD.
CONCLUSIONS/SIGNIFICANCE: Our results show discrepancies between the two classifications, including misclassification of severe dengue cases as mild cases by the WHO 1997 classification. Using an adapted WHO 2009 classification, SD more precisely defines the group of patients requiring careful clinical care at a given time during hospitalization.
世界卫生组织(WHO)于 1997 年和 2009 年分别提出了登革热临床分类指南,以指导患者的临床管理。1997 年的 WHO 分类根据严重程度将登革热感染分为三类:登革热(DF)、登革出血热(DHF)和登革休克综合征(DSS)。2009 年的 WHO 替代指南提供了一种横断面分类方法,旨在将登革热与有预警症状(DWWS)和重症登革热(SD)区分开来。本研究的主要目的是比较两种登革热分类方法。次要目的是描述在疾病过程中不同严重程度的患者发生的血液学和生化参数变化,因为向更严重的临床形式进展是不可预测的。
方法/主要发现:我们在柬埔寨进行了一项前瞻性、单中心、横断面研究,纳入了 243 名年龄在 2 至 15 岁的患有严重和非严重登革热的住院儿童。我们使用定量逆转录 PCR 或 NS1 抗原捕获 ELISA 确诊了 71.2%的急性登革样疾病患者,其中 87.2%和 9.0%的 DF 病例分别被归类为 DWWS 和 SD,35.9%的 DHF 根据适应的 2009 年 WHO SD 病例定义归类为 SD。入院时系统使用超声对于发现血浆渗漏至关重要。不同登革热严重程度组之间分泌的 NS1 蛋白浓度没有差异。DWWS 和 SD 入院时的血脂谱不同,SD 患者总胆固醇、高密度脂蛋白胆固醇和低密度脂蛋白胆固醇降低。
结论/意义:我们的结果表明,两种分类方法存在差异,包括 1997 年的 WHO 分类将重症登革热病例错误地归类为轻症病例。使用适应的 2009 年 WHO 分类,SD 更准确地定义了在住院期间某个特定时间需要密切临床护理的患者群体。