Infectious Diseases Unit, Hospital Infantil Manuel de Jesús Rivera, Managua, Nicaragua.
PLoS Negl Trop Dis. 2011 Nov;5(11):e1397. doi: 10.1371/journal.pntd.0001397. Epub 2011 Nov 8.
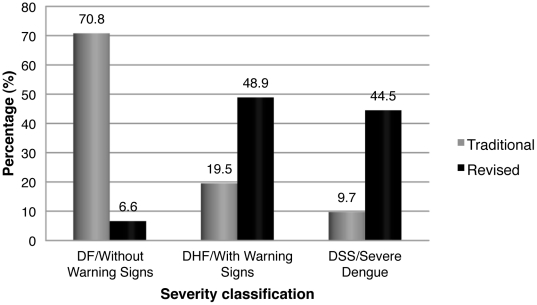
Dengue is a major public health problem worldwide and continues to increase in incidence. Dengue virus (DENV) infection leads to a range of outcomes, including subclinical infection, undifferentiated febrile illness, Dengue Fever (DF), life-threatening syndromes with fluid loss and hypotensive shock, or other severe manifestations such as bleeding and organ failure. The long-standing World Health Organization (WHO) dengue classification and management scheme was recently revised, replacing DF, Dengue Hemorrhagic Fever (DHF), and Dengue Shock Syndrome (DSS) with Dengue without Warning Signs, Dengue with Warning Signs (abdominal pain, persistent vomiting, fluid accumulation, mucosal bleeding, lethargy, liver enlargement, increasing hematocrit with decreasing platelets) and Severe Dengue (SD; dengue with severe plasma leakage, severe bleeding, or organ failure). We evaluated the traditional and revised classification schemes against clinical intervention levels to determine how each captures disease severity using data from five years (2005-2010) of a hospital-based study of pediatric dengue in Managua, Nicaragua. Laboratory-confirmed dengue cases (n = 544) were categorized using both classification schemes and by level of care (I-III). Category I was out-patient care, Category II was in-patient care that did not meet criteria for Category III, which included ICU admission, ventilation, administration of inotropic drugs, or organ failure. Sensitivity and specificity to capture Category III care for DHF/DSS were 39.0% and 75.5%, respectively; sensitivity and specificity for SD were 92.1% and 78.5%, respectively. In this data set, DENV-2 was found to be significantly associated with DHF/DSS; however, this association was not observed with the revised classification. Among dengue-confirmed cases, the revised WHO classification for severe dengue appears to have higher sensitivity and specificity to identify cases in need of heightened care, although it is no longer as specific for a particular pathogenic entity as was the traditional schema.
登革热是全球主要的公共卫生问题,发病率持续上升。登革病毒(DENV)感染可导致多种结局,包括无症状感染、非特异性发热、登革热(DF)、伴有体液丢失和低血压性休克的危及生命综合征,或其他严重表现,如出血和器官衰竭。世界卫生组织(WHO)长期以来的登革热分类和管理方案最近进行了修订,用无警告症状登革热、有警告症状登革热(腹痛、持续呕吐、体液蓄积、黏膜出血、嗜睡、肝肿大、血小板减少伴血细胞比容升高)和重症登革热(SD;严重血浆渗漏、严重出血或器官衰竭的登革热)取代 DF、登革出血热(DHF)和登革休克综合征(DSS)。我们评估了传统和修订的分类方案与临床干预水平的关系,以确定这两种方案如何使用尼加拉瓜马那瓜一家医院 5 年(2005-2010 年)的儿科登革热研究数据来捕捉疾病的严重程度。实验室确诊的登革热病例(n=544)分别使用两种分类方案和护理级别(I-III)进行分类。I 级为门诊治疗,II 级为不符合 III 级标准的住院治疗,包括入住 ICU、通气、给予正性肌力药物或器官衰竭。DHF/DSS 级别的 III 级治疗的敏感性和特异性分别为 39.0%和 75.5%,SD 的敏感性和特异性分别为 92.1%和 78.5%。在本数据集中,发现 DENV-2 与 DHF/DSS 显著相关;然而,这种关联在修订后的分类中没有观察到。在登革热确诊病例中,修订后的 WHO 重症登革热分类方案似乎对需要加强护理的病例具有更高的敏感性和特异性,尽管它对特定的病原体实体不再像传统方案那样具有特异性。