Institute for International Programs, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Center for Child and Community Health Research, Department of Pediatrics, Johns Hopkins School of Medicine, Baltimore, MD, USA.
BMC Pregnancy Childbirth. 2020 Sep 14;20(1):534. doi: 10.1186/s12884-020-03220-3.
Nigeria is the largest country in sub-Saharan Africa, with one of the highest neonatal mortality rates and the second highest number of neonatal deaths in the world. There is broad international consensus on which interventions can most effectively reduce neonatal mortality, however, there is little direct evidence on what interventions are effective in the Nigerian setting.
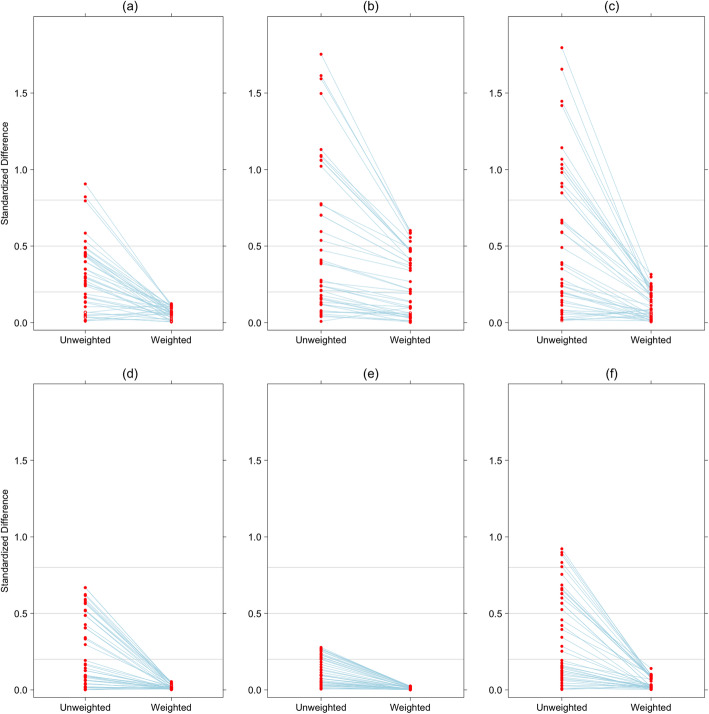
We used the 2013 Nigeria Demographic and Health Survey (NDHS) and the follow-up 2014 Verbal and Social Autopsy study of neonatal deaths to estimate the association between neonatal survival and mothers' and neonates' receipt of 18 resources and interventions along the continuum of care with information available in the NDHS. We formed propensity scores to predict the probability of receiving the intervention or resource and then weighted the observations by the inverse of the propensity score to estimate the association with mortality. We examined all-cause mortality as well as mortality due to infectious causes and intrapartum related events.
Among 19,685 livebirths and 538 neonatal deaths, we achieved adequate balance for population characteristics and maternal and neonatal health care received for 10 of 18 resources and interventions, although inference for most antenatal interventions was not possible. Of ten resources and interventions that met our criteria for balance of potential confounders, only early breastfeeding was related to decreased all-cause neonatal mortality (relative risk 0.42, 95% CI 0.32-0.52, p < 0.001). Maternal decision making and postnatal health care reduced mortality due to infectious causes, with relative risks of 0.29 (95% CI 0.09-0.88; 0.030) and 0.46 (0.22-0.95; 0.037), respectively. Early breastfeeding and delayed bathing were related to decreased mortality due to intrapartum events, although these are not likely to be causal associations.
Access to immediate postnatal care and women's autonomous decision-making have been among the most effective interventions for reducing neonatal mortality in Nigeria. As neonatal mortality increases relative to overall child mortality, accessible interventions are necessary to make further progress for neonatal survival in Nigeria and other low resource settings.
尼日利亚是撒哈拉以南非洲最大的国家,其新生儿死亡率居世界第二,新生儿死亡人数居世界第二。国际上广泛认为,哪些干预措施最能有效地降低新生儿死亡率,但在尼日利亚的具体环境下,哪种干预措施有效,几乎没有直接证据。
我们使用了 2013 年尼日利亚人口与健康调查(NDHS)和 2014 年新生儿口头和社会死因研究随访数据来估计新生儿生存与母亲和新生儿在整个护理过程中获得 18 种资源和干预措施之间的关联,这些信息都可以从 NDHS 中获得。我们形成倾向得分来预测接受干预或资源的概率,然后根据倾向得分的倒数对观察结果进行加权,以估计与死亡率的关联。我们检查了所有原因的死亡率以及由感染原因和分娩期相关事件导致的死亡率。
在 19685 例活产和 538 例新生儿死亡中,我们为 18 种资源和干预措施中的 10 种实现了人口特征和母婴保健服务获得情况的充分平衡,尽管大多数产前干预的推断是不可能的。在满足我们对潜在混杂因素平衡标准的十种资源和干预措施中,只有早期母乳喂养与全因新生儿死亡率降低有关(相对风险 0.42,95%CI 0.32-0.52,p<0.001)。产妇决策和产后保健可降低由感染原因导致的死亡率,相对风险分别为 0.29(95%CI 0.09-0.88;0.030)和 0.46(0.22-0.95;0.037)。早期母乳喂养和延迟洗澡与分娩期相关事件导致的死亡率降低有关,但这些可能不是因果关系。
在尼日利亚,获得即时产后护理和妇女自主决策一直是降低新生儿死亡率最有效的干预措施之一。随着新生儿死亡率相对于儿童总体死亡率的上升,在尼日利亚和其他资源匮乏的环境中,为新生儿生存取得进一步进展,需要采取可行的干预措施。