Yoon Ji-Young, Park Chul-Gue, Kim Eun-Jung, Choi Byung-Moon, Yoon Ji-Uk, Kim Yeon Ha, Lee Moon Ok, Han Ki Seob, Ahn Ji-Hye
Department of Dental Anesthesia and Pain Medicine, School of Dentistry, Pusan National University, Dental Research Institute, Yangsan, Republic of Korea.
Department of Anesthesiology and Pain Medicine, Asan Medical Centre, University of Ulsan College of Medicine, Seoul, Republic of Korea.
J Dent Anesth Pain Med. 2020 Aug;20(4):195-202. doi: 10.17245/jdapm.2020.20.4.195. Epub 2020 Aug 27.
Nasotracheal intubation is the most commonly used method to secure the field of view when performing surgery on the oral cavity or neck. Like orotracheal intubation, nasotracheal intubation uses a laryngoscope. Hemodynamic change occurs due to the stimulation of the sympathetic nervous system. Recently, video laryngoscope with a camera attached to the end of the direct laryngoscope blade has been used to minimize this change. In this study, we investigated the optimal effect-site concentration (Ce) of remifentanil for minimizing hemodynamic responses during nasotracheal intubation with a video laryngoscope.
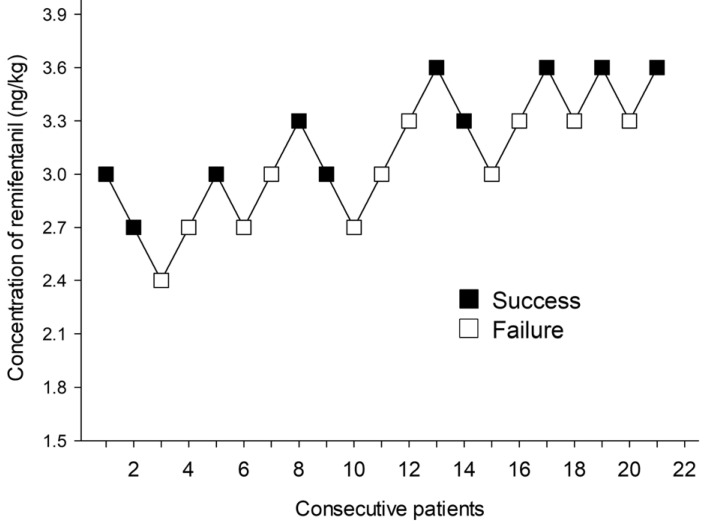
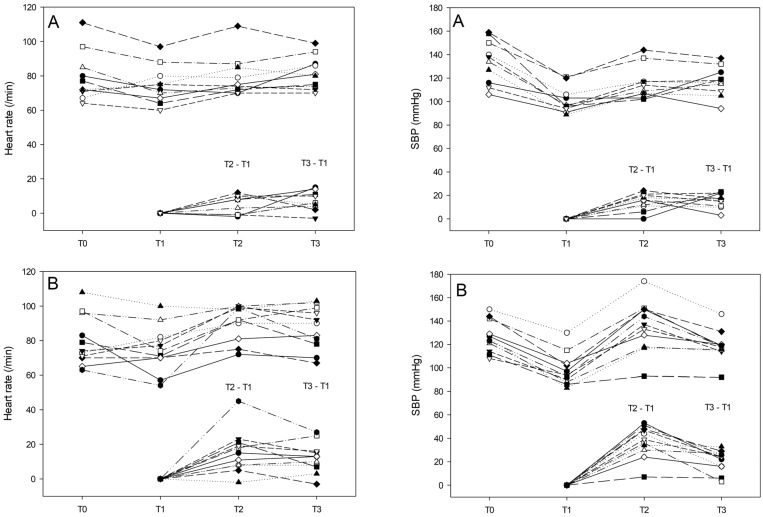
Twenty-one patients, aged between 19 and 60 years old, scheduled for elective surgery were included in this study. Anesthesia was induced by slowly injecting propofol. At the same time, remifentanil infusion was initiated at 3.0 ng/ml via target-controlled infusion (TCI). When remifentanil attained the preset Ce, nasotracheal intubation was performed using a video laryngoscope. The patient's blood pressure and heart rate were checked pre-induction, right before and after intubation, and 1 min after intubation. Hemodynamic stability was defined as an increase in systolic blood pressure and heart rate by 20% before and after nasotracheal intubation. The response of each patient determined the Ce of remifentanil for the next patient at an interval of 0.3 ng/ml.
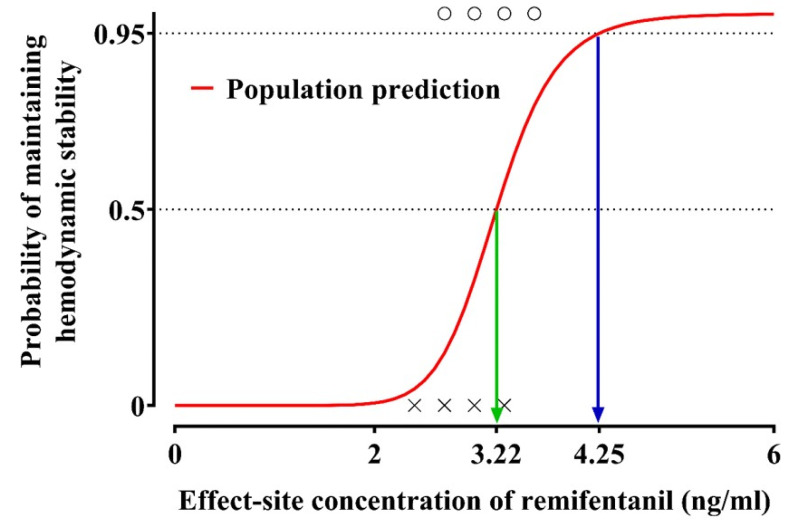
The of remifentanil administered ranged from 2.4 to 3.6 ng/ml for the patients evaluated. The estimated optimal effective effect-site concentrations of remifentanil were 3.22 and 4.25 ng/ml, that were associated with a 50% and 95% probability of maintaining hemodynamic stability, respectively.
Nasotracheal intubation using a video laryngoscope can be successfully performed in a hemodynamically stable state by using the optimal remifentanil effect-site concentration ( , 3.22 ng/ml; , 4.25 ng/ml).
在进行口腔或颈部手术时,鼻气管插管是确保视野的最常用方法。与口气管插管一样,鼻气管插管也使用喉镜。由于交感神经系统受到刺激,会发生血流动力学变化。最近,在直接喉镜叶片末端连接摄像头的视频喉镜已被用于尽量减少这种变化。在本研究中,我们调查了瑞芬太尼的最佳效应室浓度(Ce),以尽量减少使用视频喉镜进行鼻气管插管期间的血流动力学反应。
本研究纳入了21例年龄在19至60岁之间、计划进行择期手术的患者。通过缓慢注射丙泊酚诱导麻醉。同时,通过靶控输注(TCI)以3.0 ng/ml的速度开始输注瑞芬太尼。当瑞芬太尼达到预设的Ce时,使用视频喉镜进行鼻气管插管。在诱导前、插管前后及插管后1分钟检查患者的血压和心率。血流动力学稳定性定义为鼻气管插管前后收缩压和心率升高20%。每个患者的反应决定下一个患者瑞芬太尼的Ce,间隔为0.3 ng/ml。
评估的患者瑞芬太尼给药浓度范围为2.4至3.6 ng/ml。瑞芬太尼的估计最佳有效效应室浓度分别为3.22和4.25 ng/ml,分别与维持血流动力学稳定性的50%和95%概率相关。
使用最佳瑞芬太尼效应室浓度(Ce50,3.22 ng/ml;Ce95,4.25 ng/ml),可以在血流动力学稳定状态下成功进行使用视频喉镜的鼻气管插管。