Breast Cancer Now Toby Robins Research Centre, The Institute of Cancer Research, London, UK.
Breast Unit, Royal Marsden Hospital, London, UK.
J Natl Cancer Inst. 2021 Mar 1;113(3):309-317. doi: 10.1093/jnci/djaa087.
There are no established molecular biomarkers for patients with breast cancer receiving combination endocrine and CDK4/6 inhibitor (CDK4/6i). We aimed to determine whether genomic markers in circulating tumor DNA (ctDNA) can identify patients at higher risk of early progression on fulvestrant therapy with or without palbociclib, a CDK4/6i.
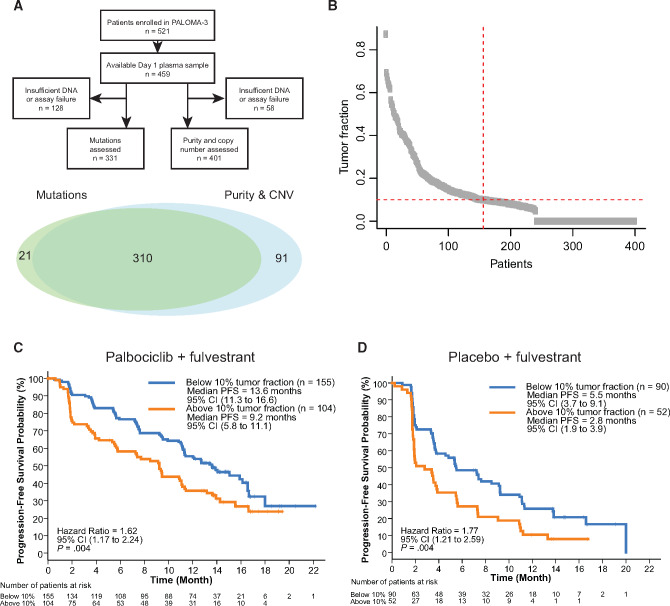
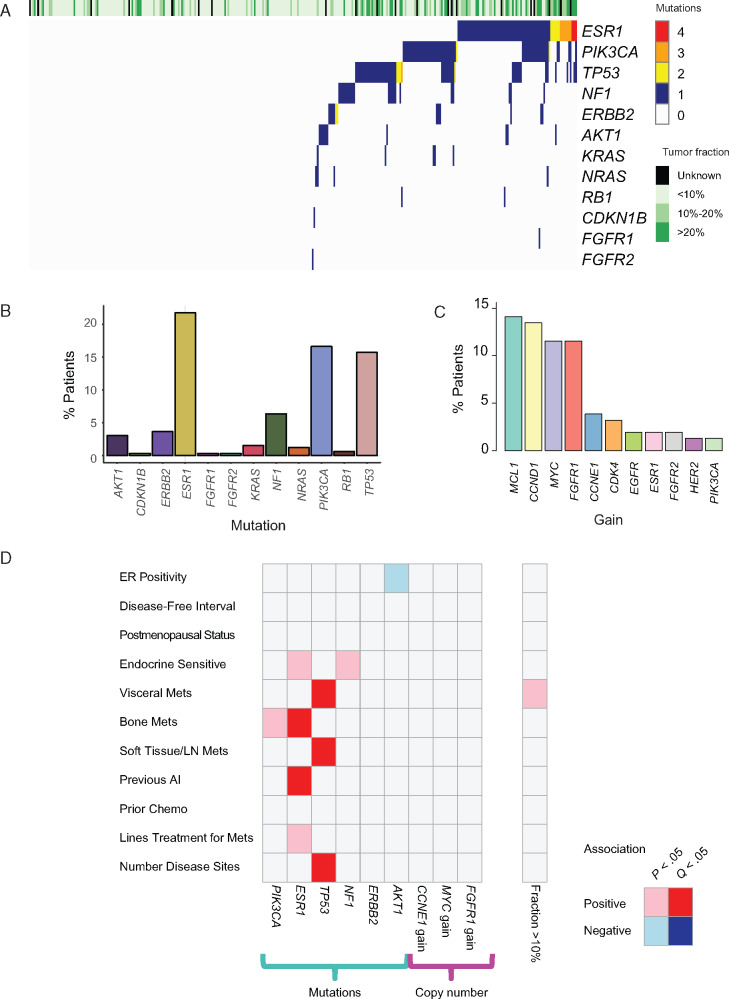
PALOMA-3 was a phase III, multicenter, double-blind randomized controlled trial of palbociclib plus fulvestrant (n = 347) vs placebo plus fulvestrant (n = 174) in patients with endocrine-pretreated estrogen receptor-positive (ER+) breast cancer. Pretreatment plasma samples from 459 patients were analyzed for mutations in 17 genes, copy number in 14 genes, and circulating tumor fraction. Progression-free survival (PFS) was compared in patients with circulating tumor fraction above or below a prespecified cutoff of 10% and with or without a specific genomic alteration. All statistical tests were 2-sided.
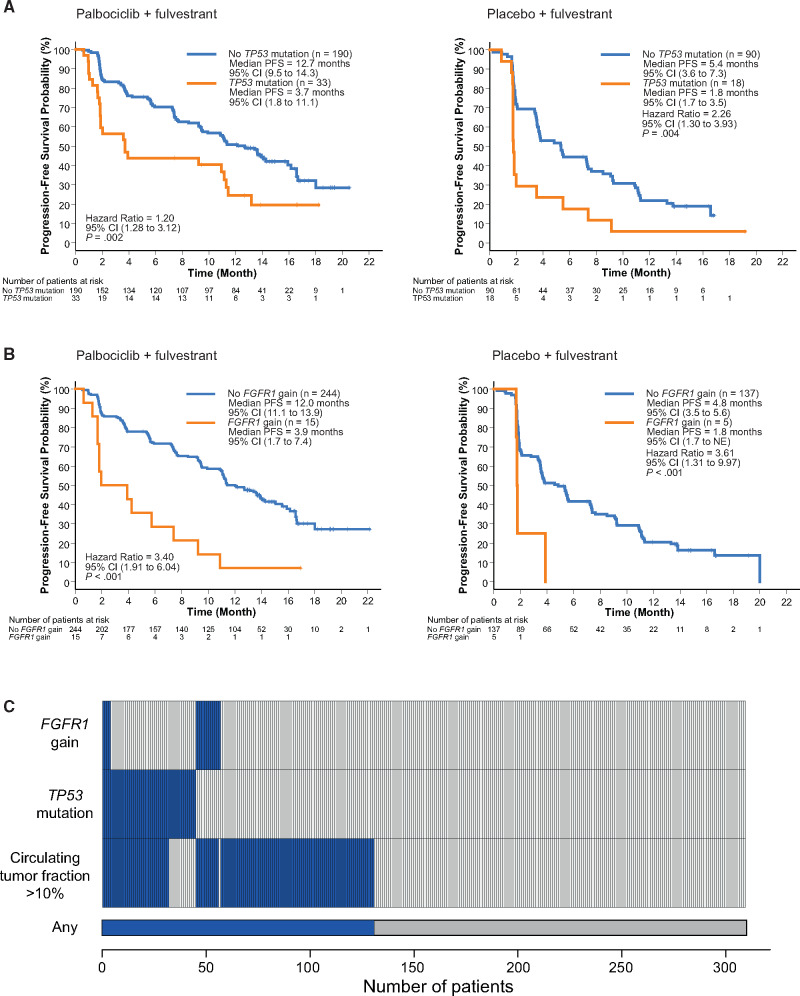
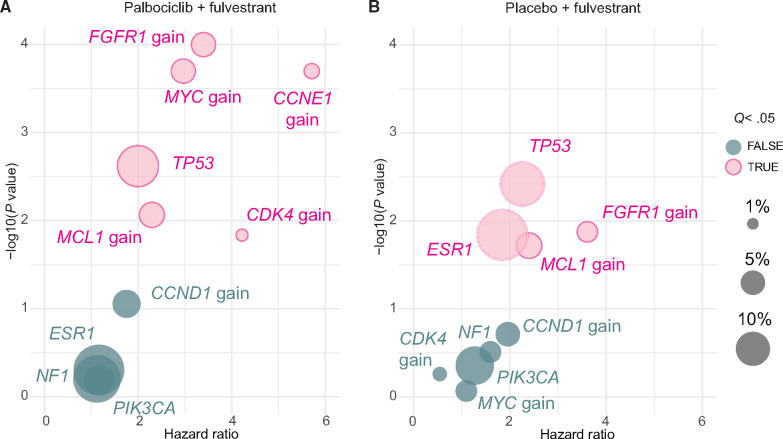
Patients with high ctDNA fraction had worse PFS on both palbociclib plus fulvestrant (hazard ratio [HR] = 1.62, 95% confidence interval [CI] = 1.17 to 2.24; P = .004) and placebo plus fulvestrant (HR = 1.77, 95% CI = 1.21 to 2.59; P = .004). In multivariable analysis, high-circulating tumor fraction was associated with worse PFS (HR = 1.20 per 10% increase in tumor fraction, 95% CI = 1.09 to 1.32; P < .001), as was TP53 mutation (HR = 1.84, 95% CI = 1.27 to 2.65; P = .001) and FGFR1 amplification (HR = 2.91, 95% CI = 1.61 to 5.25; P < .001). No interaction with treatment randomization was observed.
Pretreatment ctDNA identified a group of high-risk patients with poor clinical outcome despite the addition of CDK4/6 inhibition. These patients might benefit from inclusion in future trials of escalating treatment, with therapies that may be active in these genomic contexts.
目前尚无针对接受联合内分泌和 CDK4/6 抑制剂(CDK4/6i)治疗的乳腺癌患者的明确分子生物标志物。我们旨在确定循环肿瘤 DNA(ctDNA)中的基因组标志物是否可以识别出在接受氟维司群联合或不联合 CDK4/6i 帕博西利治疗时早期进展风险较高的患者。
PALOMA-3 是一项 III 期、多中心、双盲、随机对照试验,比较了氟维司群联合帕博西利(n=347)与安慰剂联合氟维司群(n=174)治疗内分泌预处理的雌激素受体阳性(ER+)乳腺癌患者的疗效。对 459 名患者的预处理血浆样本进行了 17 个基因的突变分析、14 个基因的拷贝数分析和循环肿瘤分数分析。比较了循环肿瘤分数高于或低于预设 10%截断值的患者以及存在或不存在特定基因组改变的患者的无进展生存期(PFS)。所有统计检验均为双侧检验。
高 ctDNA 分数的患者在接受氟维司群联合帕博西利(HR=1.62,95%CI=1.17 至 2.24;P=0.004)和安慰剂联合氟维司群(HR=1.77,95%CI=1.21 至 2.59;P=0.004)治疗时的 PFS 更差。多变量分析显示,高循环肿瘤分数与较差的 PFS 相关(HR=1.20/肿瘤分数增加 10%,95%CI=1.09 至 1.32;P<0.001),TP53 突变(HR=1.84,95%CI=1.27 至 2.65;P=0.001)和 FGFR1 扩增(HR=2.91,95%CI=1.61 至 5.25;P<0.001)也是如此。未观察到与治疗随机分组的相互作用。
尽管添加 CDK4/6 抑制,但治疗前 ctDNA 可识别出一组临床结局较差的高危患者。这些患者可能受益于纳入未来的治疗升级试验,采用可能在这些基因组背景下有效的治疗方法。