Department of Neurosurgery, University of Rochester Medical Center, Rochester, New York, United States of America.
Department of Neurosurgery, Huashan Hospital, Fudan University, Shanghai, China.
PLoS One. 2020 Sep 17;15(9):e0235273. doi: 10.1371/journal.pone.0235273. eCollection 2020.
Sepsis and septic shock are important quality and patient safety metrics. This study examines incidence of Sepsis and/or septic shock (S/SS) after craniotomy for tumor resection, one of the most common neurosurgical operations.
Multicenter, prospectively collected data from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was used to identify patients undergoing craniotomy for tumor (CPT 61510, 61521, 61520, 61518, 61526, 61545, 61546, 61512, 61519, 61575) from 2012-2015. Univariate and multivariate logistic regression models were used to identify risk factors for S/SS.
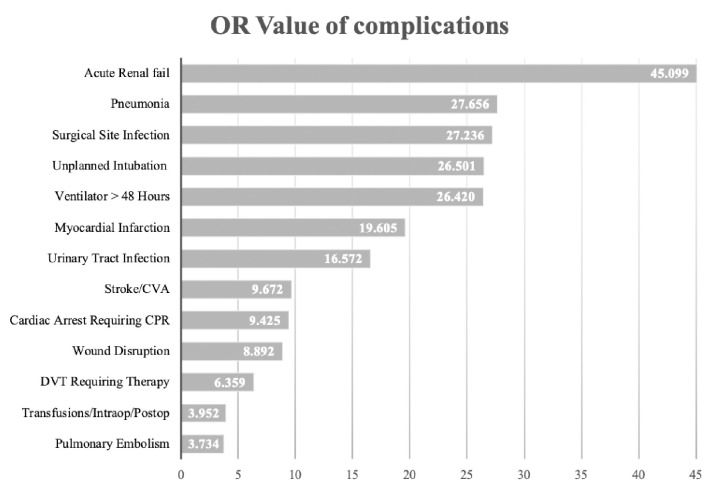
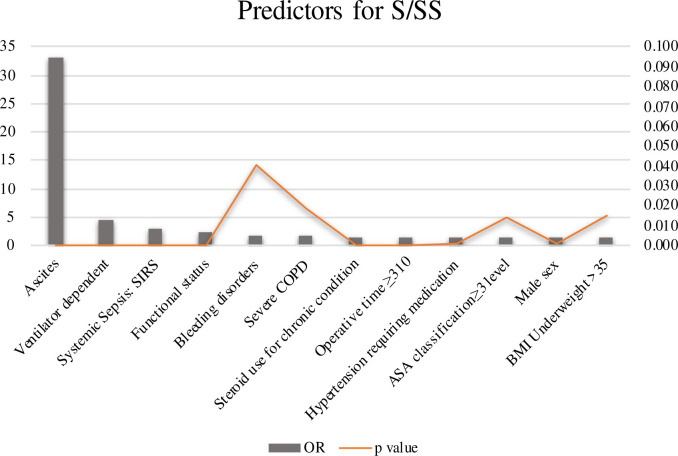
There were 18,642 patients that underwent craniotomy for tumor resection. The rate of sepsis was 1.35% with a mortality rate of 11.16% and the rate of septic shock was 0.65% with a 33.06% mortality rate versus an overall mortality rate of 2.46% in the craniotomy for tumor cohort. The 30-day readmission rate was 50.54% with S/SS vs 10.26% in those without S/SS. Multiple factors were identified as statistically significant (p <0.05) for S/SS including ascites (OR = 33.0), ventilator dependence (OR = 4.5), SIRS (OR = 2.8), functional status (OR = 2.3), bleeding disorders (OR = 1.7), severe COPD (OR = 1.6), steroid use (OR = 1.6), operative time >310 minutes (OR = 1.5), hypertension requiring medication (OR = 1.5), ASA class ≥ 3 (OR = 1.4), male sex (OR = 1.4), BMI >35 (OR = 1.4) and infratentorial location.
The data indicate that sepsis and septic shock, although uncommon after craniotomy for tumor resection, carry a significant risk of 30-day unplanned reoperation (35.60%) and mortality (18.21%). The most significant risk factors are ventilator dependence, ascites, SIRS and poor functional status. By identifying the risk factors for S/SS, neurosurgeons can potentially improve outcomes. Further investigation should focus on the creation of a predictive score for S/SS with integration into the electronic health record for targeted protocol initiation in this unique neurosurgical patient population.
脓毒症和感染性休克是重要的质量和患者安全指标。本研究调查了颅脑肿瘤切除术(最常见的神经外科手术之一)后发生脓毒症和/或感染性休克(S/SS)的发生率。
使用美国外科医师学会国家外科质量改进计划(ACS NSQIP)数据库的多中心前瞻性收集的数据,确定 2012 年至 2015 年间接受颅脑肿瘤切除术(CPT 61510、61521、61520、61518、61526、61545、61546、61512、61519、61575)的患者。使用单变量和多变量逻辑回归模型确定 S/SS 的危险因素。
共有 18642 例患者接受颅脑肿瘤切除术。脓毒症的发生率为 1.35%,死亡率为 11.16%,感染性休克的发生率为 0.65%,死亡率为 33.06%,而颅脑肿瘤组的总死亡率为 2.46%。颅脑肿瘤组 30 天再入院率为 50.54%,S/SS 组为 33.0%,无 S/SS 组为 10.26%。多个因素被确定为 S/SS 的统计学显著(p<0.05),包括腹水(OR=33.0)、呼吸机依赖(OR=4.5)、全身炎症反应综合征(SIRS)(OR=2.8)、功能状态(OR=2.3)、出血性疾病(OR=1.7)、严重 COPD(OR=1.6)、类固醇使用(OR=1.6)、手术时间>310 分钟(OR=1.5)、需要药物治疗的高血压(OR=1.5)、ASA 分级≥3(OR=1.4)、男性(OR=1.4)、BMI>35(OR=1.4)和幕下位置。
数据表明,尽管颅脑肿瘤切除术后脓毒症和感染性休克并不常见,但仍存在 30 天计划外再次手术(35.60%)和死亡(18.21%)的显著风险。最显著的危险因素是呼吸机依赖、腹水、SIRS 和功能状态差。通过确定 S/SS 的危险因素,神经外科医生可以潜在地改善结果。进一步的研究应集中于创建 S/SS 的预测评分,并将其整合到电子健康记录中,以便在这一独特的神经外科患者群体中针对特定协议进行启动。