Division of Psychiatry, University College London, United Kingdom.
King's College London, Institute of Psychiatry, Psychology and Neuroscience, London, United Kingdom.
PLoS Med. 2020 Sep 17;17(9):e1003306. doi: 10.1371/journal.pmed.1003306. eCollection 2020 Sep.
The higher mortality rates in people with severe mental illness (SMI) may be partly due to inadequate integration of physical and mental healthcare. Accurate recording of SMI during hospital admissions has the potential to facilitate integrated care including tailoring of treatment to account for comorbidities. We therefore aimed to investigate the sensitivity of SMI recording within general hospitals, changes in diagnostic accuracy over time, and factors associated with accurate recording.
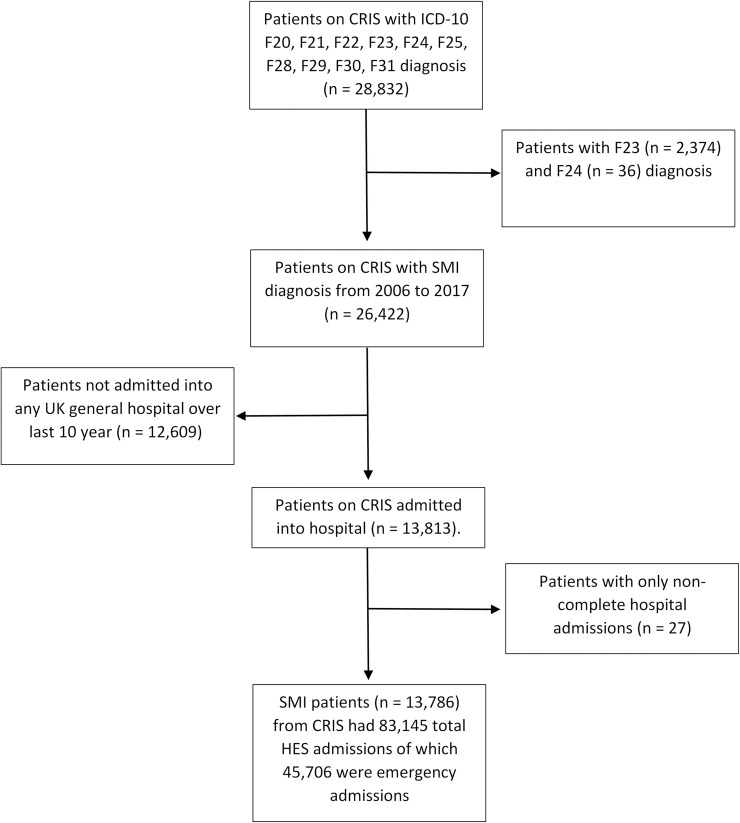
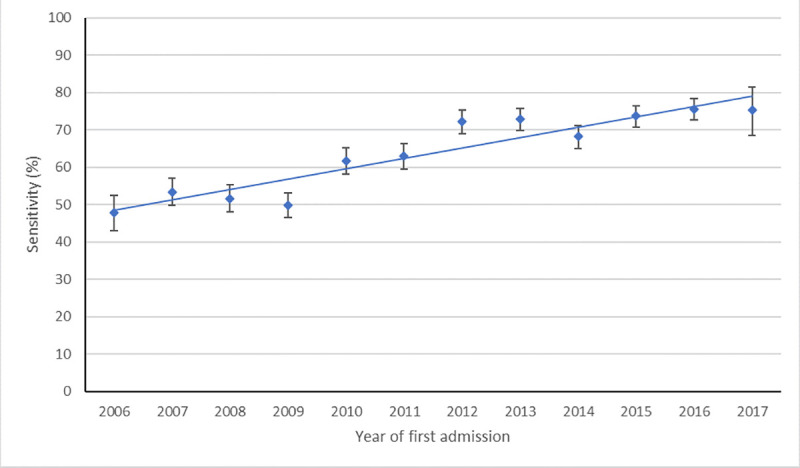
We undertook a cohort study of 13,786 adults with SMI diagnosed during 2006-2017, using data from a large secondary mental healthcare database as reference standard, linked to English national records for 45,706 emergency hospital admissions. We examined general hospital record sensitivity across patients' subsequent hospital records, for each subsequent emergency admission, and at different levels of diagnostic precision. We analyzed time trends during the study period and used logistic regression to examine sociodemographic and clinical factors associated with psychiatric recording accuracy, with multiple imputation for missing data. Sensitivity for recording of SMI as any mental health diagnosis was 76.7% (95% CI 76.0-77.4). Category-level sensitivity (e.g., proportion of individuals with schizophrenia spectrum disorders (F20-29) who received any F20-29 diagnosis in hospital records) was 56.4% (95% CI 55.4-57.4) for schizophrenia spectrum disorder and 49.7% (95% CI 48.1-51.3) for bipolar affective disorder. Sensitivity for SMI recording in emergency admissions increased from 47.8% (95% CI 43.1-52.5) in 2006 to 75.4% (95% CI 68.3-81.4) in 2017 (ptrend < 0.001). Minority ethnicity, being married, and having better mental and physical health were associated with less accurate diagnostic recording. The main limitation of our study is the potential for misclassification of diagnosis in the reference-standard mental healthcare data.
Our findings suggest that there have been improvements in recording of SMI diagnoses, but concerning under-recording, especially in minority ethnic groups, persists. Training in culturally sensitive diagnosis, expansion of liaison psychiatry input in general hospitals, and improved data sharing between physical and mental health services may be required to reduce inequalities in diagnostic practice.
严重精神疾病(SMI)患者的死亡率较高,部分原因可能是身心保健整合不足。在住院期间准确记录 SMI 有潜力促进综合护理,包括针对合并症调整治疗。因此,我们旨在调查综合医院中 SMI 记录的敏感性、随时间变化的诊断准确性变化,以及与准确记录相关的因素。
我们对 2006 年至 2017 年间确诊的 13786 名 SMI 成年患者进行了队列研究,使用来自大型二级精神卫生保健数据库的数据作为参考标准,与英格兰全国 45706 例紧急住院记录相链接。我们检查了患者随后的住院记录、每次随后的紧急入院记录以及不同诊断精度水平下综合医院记录的敏感性。我们分析了研究期间的时间趋势,并使用逻辑回归分析了与精神科记录准确性相关的社会人口学和临床因素,对缺失数据进行了多重插补。记录任何心理健康诊断的 SMI 的敏感性为 76.7%(95%CI 76.0-77.4)。类别水平敏感性(例如,精神分裂症谱系障碍(F20-29)患者中有多少人在医院记录中接受了任何 F20-29 诊断),精神分裂症谱系障碍为 56.4%(95%CI 55.4-57.4),双相情感障碍为 49.7%(95%CI 48.1-51.3)。2006 年急诊入院 SMI 记录的敏感性为 47.8%(95%CI 43.1-52.5),2017 年为 75.4%(95%CI 68.3-81.4)(ptrend <0.001)。少数民族、已婚和更好的精神和身体健康与不太准确的诊断记录相关。我们研究的主要限制是参考标准精神保健数据中诊断可能存在分类错误。
我们的研究结果表明,在记录 SMI 诊断方面有所改善,但令人担忧的是,尤其是在少数民族群体中,记录不足的情况仍然存在。可能需要进行文化敏感诊断培训、扩大综合医院联络精神病学投入以及改善身心健康服务之间的数据共享,以减少诊断实践中的不平等。