Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong SAR, China.
Department of Medicine, University of Toronto, Canada.
PLoS Med. 2020 Sep 18;17(9):e1003316. doi: 10.1371/journal.pmed.1003316. eCollection 2020 Sep.
Lifetime glycemic exposure and its relationship with age at diagnosis in type 2 diabetes (T2D) are unknown. Pharmacologic glycemic management strategies for young-onset T2D (age at diagnosis <40 years) are poorly defined. We studied how age at diagnosis affects glycemic exposure, glycemic deterioration, and responses to oral glucose-lowering drugs (OGLDs).
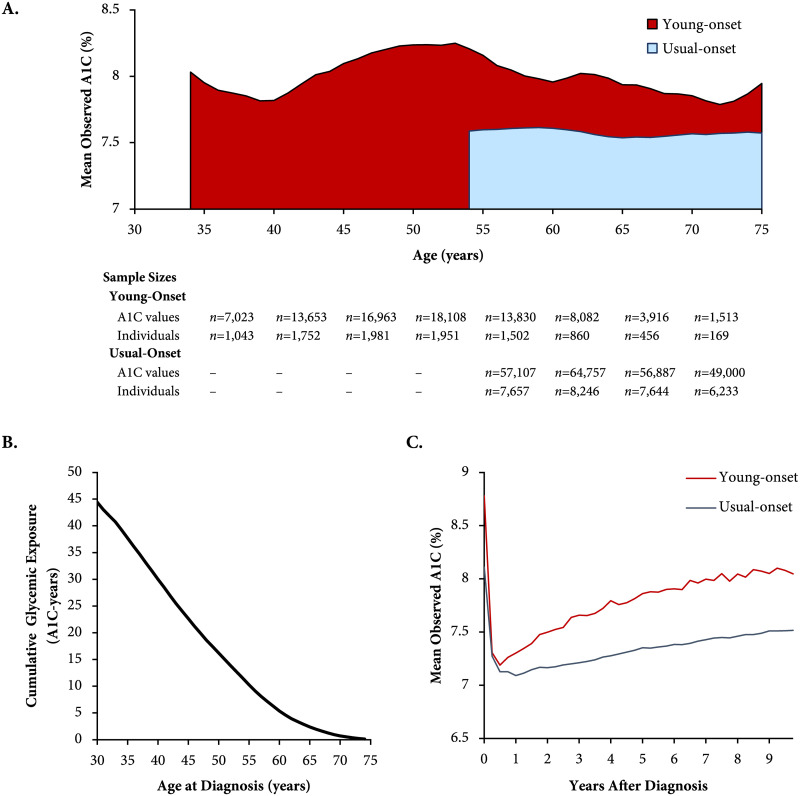
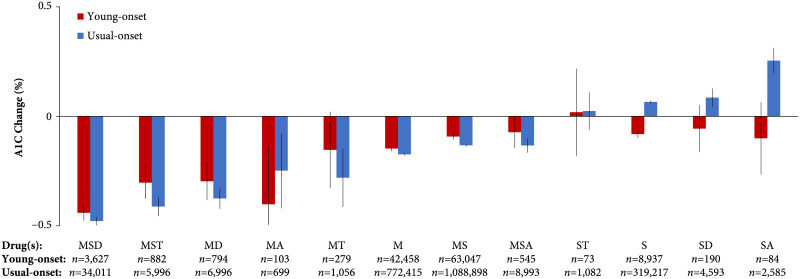
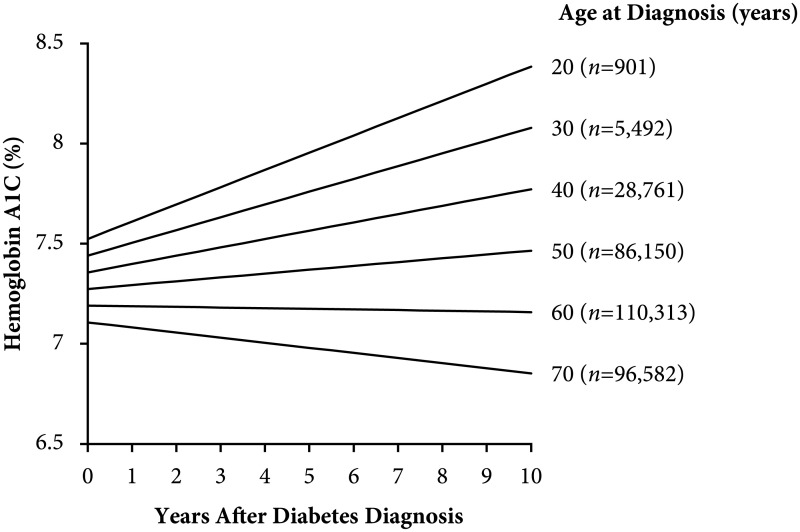
In a population-based cohort (n = 328,199; 47.2% women; mean age 34.6 and 59.3 years, respectively, for young-onset and usual-onset [age at diagnosis ≥40 years] T2D; 2002-2016), we used linear mixed-effects models to estimate the association between age at diagnosis and A1C slope (glycemic deterioration) and tested for an interaction between age at diagnosis and responses to various combinations of OGLDs during the first decade after diagnosis. In a register-based cohort (n = 21,016; 47.1% women; mean age 43.8 and 58.9 years, respectively, for young- and usual-onset T2D; 2000-2015), we estimated the glycemic exposure from diagnosis until age 75 years. People with young-onset T2D had a higher mean A1C (8.0% [standard deviation 0.15%]) versus usual-onset T2D (7.6% [0.03%]) throughout the life span (p < 0.001). The cumulative glycemic exposure was >3 times higher for young-onset versus usual-onset T2D (41.0 [95% confidence interval 39.1-42.8] versus 12.1 [11.8-12.3] A1C-years [1 A1C-year = 1 year with 8% average A1C]). Younger age at diagnosis was associated with faster glycemic deterioration (A1C slope over time +0.08% [0.078-0.084%] per year for age at diagnosis 20 years versus +0.02% [0.016-0.018%] per year for age at diagnosis 50 years; p-value for interaction <0.001). Age at diagnosis ≥60 years was associated with glycemic improvement (-0.004% [-0.005 to -0.004%] and -0.02% [-0.027 to -0.0244%] per year for ages 60 and 70 years at diagnosis, respectively; p-value for interaction <0.001). Responses to OGLDs differed by age at diagnosis (p-value for interaction <0.001). Those with young-onset T2D had smaller A1C decrements for metformin-based combinations versus usual-onset T2D (metformin alone: young-onset -0.15% [-0.105 to -0.080%], usual-onset -0.17% [-0.179 to -0.169%]; metformin, sulfonylurea, and dipeptidyl peptidase-4 inhibitor: young-onset -0.44% [-0.476 to -0.405%], usual-onset -0.48% [-0.498 to -0.459%]; metformin and α-glucosidase inhibitor: young-onset -0.40% [-0.660 to -0.144%], usual-onset -0.25% [-0.420 to -0.077%]) but greater responses to other combinations containing sulfonylureas (sulfonylurea alone: young-onset -0.08% [-0.099 to -0.065%], usual-onset +0.06% [+0.059 to +0.072%]; sulfonylurea and α-glucosidase inhibitor: young-onset -0.10% [-0.266 to 0.064%], usual-onset: 0.25% [+0.196% to +0.312%]). Limitations include possible residual confounding and unknown generalizability outside Hong Kong.
In this study, we observed excess glycemic exposure and rapid glycemic deterioration in young-onset T2D, indicating that improved treatment strategies are needed in this setting. The differential responses to OGLDs between young- and usual-onset T2D suggest that better disease classification could guide personalized therapy.
终身血糖暴露及其与 2 型糖尿病(T2D)发病年龄的关系尚不清楚。对于发病年龄<40 岁的年轻起病 T2D(通常起病年龄≥40 岁),其降糖药物治疗策略尚未明确。我们研究了发病年龄如何影响血糖暴露、血糖恶化以及对口服降糖药(OGLD)的反应。
在一项基于人群的队列研究(n=328199;女性占 47.2%;发病年龄分别为 34.6 岁和 59.3 岁,分别为年轻起病和通常起病[发病年龄≥40 岁]的 T2D;2002-2016 年)中,我们使用线性混合效应模型估计发病年龄与 A1C 斜率(血糖恶化)之间的关联,并检测发病年龄与诊断后最初 10 年内各种 OGLD 组合的反应之间是否存在交互作用。在一项基于登记的队列研究(n=21016;女性占 47.1%;发病年龄分别为 43.8 岁和 58.9 岁,分别为年轻起病和通常起病的 T2D;2000-2015 年)中,我们估计了从诊断到 75 岁的血糖暴露情况。在整个生命周期中,与通常起病的 T2D 相比,年轻起病的 T2D 患者的平均 A1C(8.0%[0.15%标准差])更高(p<0.001)。与通常起病的 T2D 相比,年轻起病的 T2D 患者的累计血糖暴露量高出 3 倍以上(41.0[95%置信区间 39.1-42.8]与 12.1[11.8-12.3]A1C 年[1 A1C 年=8%平均 A1C 水平下的 1 年])。发病年龄越小,血糖恶化越快(发病年龄 20 岁时 A1C 斜率每年增加 0.08%[0.078-0.084%],发病年龄 50 岁时每年增加 0.02%[0.016-0.018%];p 值<0.001)。发病年龄≥60 岁与血糖改善相关(发病年龄 60 岁和 70 岁时,每年分别降低-0.004%[-0.005 至-0.004%]和-0.02%[-0.027 至-0.0244%];p 值<0.001)。对 OGLD 的反应因发病年龄而异(p 值<0.001)。与通常起病的 T2D 相比,年轻起病的 T2D 患者使用二甲双胍为基础的联合治疗方案时 A1C 降低幅度较小(二甲双胍单药:年轻起病组-0.15%[-0.105 至-0.080%],通常起病组-0.17%[-0.179 至-0.169%];二甲双胍、磺脲类药物和二肽基肽酶-4 抑制剂:年轻起病组-0.44%[-0.476 至-0.405%],通常起病组-0.48%[-0.498 至-0.459%];二甲双胍和 α-葡萄糖苷酶抑制剂:年轻起病组-0.40%[-0.660 至-0.144%],通常起病组-0.25%[-0.420 至-0.077%]),但对含有磺脲类药物的其他组合反应更大(磺脲类药物单药:年轻起病组-0.08%[-0.099 至-0.065%],通常起病组+0.06%[+0.059 至+0.072%];磺脲类药物和 α-葡萄糖苷酶抑制剂:年轻起病组-0.10%[-0.266 至 0.064%],通常起病组:0.25%[+0.196% 至+0.312%])。局限性包括可能存在残余混杂因素和香港以外地区的未知普遍适用性。
在这项研究中,我们观察到年轻起病的 T2D 存在血糖暴露过多和血糖恶化迅速的情况,这表明需要在该人群中制定更有效的治疗策略。年轻起病和通常起病的 T2D 对 OGLD 的反应不同提示更好的疾病分类可能有助于指导个体化治疗。