Department of Anesthesiology and Perioperative Medicine, Henan Provincial People's Hospital, People's Hospital of Zhengzhou University, Zhengzhou, Henan, China.
Department of General Surgery, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan, Taiwan.
Breast. 2020 Dec;54:70-78. doi: 10.1016/j.breast.2020.08.017. Epub 2020 Sep 7.
To use pathologic indicators to determine which patients benefit from postmastectomy radiation therapy (PMRT) for breast cancer after neoadjuvant chemotherapy (NACT) and total mastectomy (TM).
We enrolled 4236 patients with breast invasive ductal carcinoma who received NACT followed by TM. Cox regression analysis was used to calculate hazard ratios (HRs) and confidence intervals; independent predictors were controlled for or stratified in the analysis.
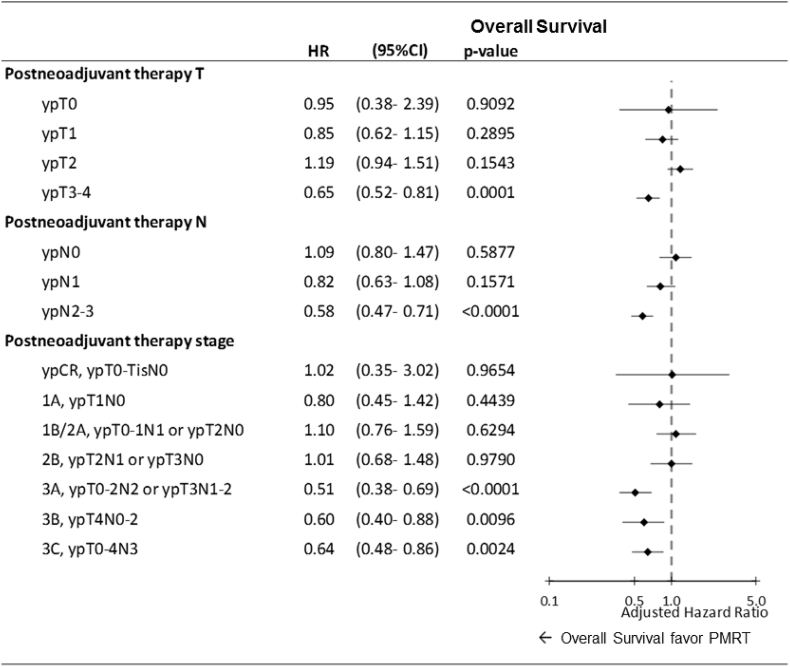
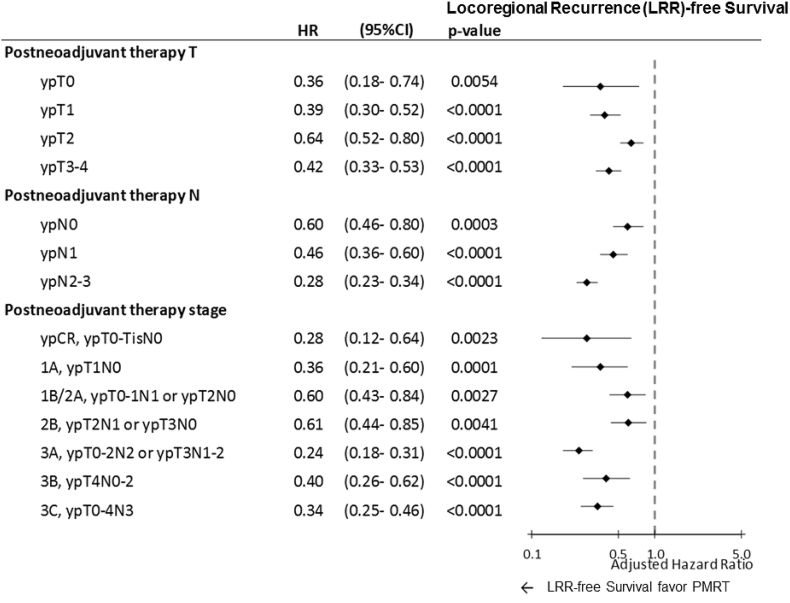
After multivariate Cox regression analyses, the adjusted HRs derived for PMRT for all-cause mortality were 0.65 (0.52-0.81, P < 0.0001) and 0.58 (0.47-0.71, P < 0.0001) in postchemotherapy pathologic tumor stages T2-4 (ypT3-4) and postchemotherapy pathologic nodal stages N2-3 (ypN2-3), respectively. Moreover, adjusted HRs derived for PMRT with all-cause mortality were 0.51 (0.38-0.69, P < 0.0001), 0.60 (0.40-0.88, P = 0.0096), and 0.64 (0.48-0.86, P = 0.0024) in pathological stages IIIA, IIIB, and IIIC, respectively. Additionally, the PMRT group showed significant locoregional control irrespective of the pathologic response, even ypT0, ypN0, or pathological complete response (pCR), compared with the No-PMRT group. The multivariate analysis showed no statistical differences between the PMRT and No-PMRT groups for distant metastasis-free survival in any pathologic response of ypT0-4, ypN0-3, and pathologic American Joint Committee on Cancer stages pCR to IIIC.
For patients with breast cancer ypT3-4, ypN2-3, or pathologic stages IIIA-IIIC receiving NACT and TM, benefit from PMRT if it is associated with OS benefits, regardless of the clinical stage of the disease. Compared with No-PMRT, PMRT improved locoregional recurrence-free survival, even pCR, in patients with breast cancer receiving NACT and TM.
利用病理指标来确定哪些接受新辅助化疗(NACT)和全乳切除术(TM)后的乳腺癌患者受益于术后放疗(PMRT)。
我们纳入了 4236 例接受 NACT 后行 TM 的乳腺浸润性导管癌患者。采用 Cox 回归分析计算风险比(HR)和置信区间;在分析中控制或分层了独立预测因素。
多变量 Cox 回归分析后,化疗后病理肿瘤分期 T2-4(ypT3-4)和化疗后病理淋巴结分期 N2-3(ypN2-3)的所有原因死亡率调整后的 PMRT 风险比分别为 0.65(0.52-0.81,P<0.0001)和 0.58(0.47-0.71,P<0.0001)。此外,所有原因死亡率调整后的 PMRT 风险比在病理分期 IIIA、IIIB 和 IIIC 中分别为 0.51(0.38-0.69,P<0.0001)、0.60(0.40-0.88,P=0.0096)和 0.64(0.48-0.86,P=0.0024)。此外,与未行 PMRT 组相比,即使在 ypT0、ypN0 或病理完全缓解(pCR)的情况下,PMRT 组也显示出显著的局部区域控制。多变量分析显示,在任何 ypT0-4、ypN0-3 和病理美国癌症联合委员会分期 pCR 至 IIIC 的病理反应中,PMRT 组和未行 PMRT 组在远处无转移生存方面无统计学差异。
对于接受 NACT 和 TM 的乳腺癌患者 ypT3-4、ypN2-3 或病理分期 IIIA-IIIC,如果与 OS 获益相关,无论疾病的临床分期如何,均可从 PMRT 中获益。与未行 PMRT 组相比,PMRT 改善了接受 NACT 和 TM 的乳腺癌患者的局部区域无复发生存,即使是 pCR。